The Bill provides for the establishment of a comprehensive health service in England and Wales. A further Bill to provide for Scotland will be introduced later.Right at the very beginning of our NHS there was a pledge to provide a service that was comprehensive and universal; available to all regardless of income or location. These principles are precious yet vulnerable. Reforms over the last two decades have chipped away at these principles and the final push to abolish them takes the form of the Coalition government's Health and Social Care Bill.
All the service, or any part of it, is to be available to everyone in England and Wales. The Bill imposes no limitation on availability – eg,. limitations on financial means, age, sex, employment or vocation, area of residence or insurance qualification.
Friday 30 December 2011
In case there is any doubt...
In 1946 the government issued a white paper describing the new NHS (Cmd 6761). The document starts with these paragraphs:
NHS Predictions for 2012
I am not a betting man so I will not put money on these predictions. Here are my fears for the coming year (I have no hopes because I can only see things getting worse).
- At some point an influential figure (whether that is a government minister, the prime minister, the CEO of a large NHS trust or a healthcare professional body) will say that NHS patients should expect to pay for cataract removal. The argument will be that patients pay for Lasik or spectacles to be able to see and this is no different, logically or morally, to having to pay for a cataract operation to see. This will be described as not being in contradiction to the NHS ethos of free-at-the-point-of-use because that principle will always apply to life threatening conditions (see what they've done there?).
- There will be a rationalisation of prescription charges. This will result in people who are being treated for cancer will find that their cancer drugs will no longer be subject to prescription charges. The flip side is that the DH will make up for the loss of prescription charges in one area by introducing them in another area. The Department will review the entire prescription charges policy and they will take the view that only essential, life-giving drugs will be exempt from prescription charges. So for example insulin will be exempt but drugs to treat hypertension - where there will be no immediate effect on mortality if the patients stopped taking the drug - will be regarded as non-essential and hence subject to prescription charges. The government will say that prescription charges for preventative drugs will reflect their policy of patients taking more responsibility for their health.
- The Francis report will be published some time early in 2012. Some parts of the Press will use it to say that the entire NHS is not fit for purpose and the BBC, as usual, will find some obscure person and quote them saying that the NHS needs a complete overhaul. Andrew Lansley will silently punch the air when he hears this on the 8am news bulletin on Radio 4. However, the significant part of the Francis report will be the sections that show how local and national Conservative politicians have exploited and conflated what happened at Mid Staffs for political gain. The question is whether there will be a backlash against those politicians.
- At some point there will be yet another scandal in care homes and CQC will be pilloried for not noticing the issues, and worse, for producing a glowing report for a clearly failing care home. Since CQC is a vital gangplank of Lansley's plans he will (yet again) make just a few derrogatory comments and leave CQC and its inadequate budget, largely unchanged. This will lay the foundations for yet more scandals in 2013.
- The Department of Health will finally do what it should have done in the Autumn of 2010 and announce a minimum population that each CCG has to cover before it will be authorised. There will be upheaval as pathfinder CCGs merge and there will be a lot of grumbling as people say that local decision making is being moved to large faceless organisations. (The counter argument that it would have been better to have left PCTs alone will be lost in the din.) In the run up to the April 2013 handover date, there will be fewer than 200 CCGs, maybe as low as, (umm) the 152 PCTs they are supposed to replace.
- The Health and Social Care Act will get Royal Assent. There will be a lot of huffing and puffing (or perhaps wheezing) in the Lords during the Report stage. There will also be heated debates in the Commons when consideration the Lords amendments. Labour, as always, will have an uncoordinated attack; Lib Dem MPs will give speeches saying, effectively, what they didn't like about the NHS under Labour but will be clueless about the effect of the Bill; and Tory MPs will say that Lansley is a god because they have been whipped to say it. If we are lucky (it's a big if) the Secretary of State will be forced to retain the responsibility for the NHS and for determining whether the NHS charges for treatment. But it is a big if.
Thursday 29 December 2011
Memories of Paul
When I was a student I shared a house with two friends, one of them was Paul. Everyone loved Paul, he was intelligent, easy-going and fun to be with. Perhaps too many people loved him, because sometimes he would request that if this girl or that girl turned up at our house, we were to tell her he wasn't in. On one occasion he insisted vociferously that we go to the pub (something we did not normally need to be persuaded) only to return to find out why: a girl he had met at a party had decided to call round, and she was so intent on seeing him that she had broken into our house and was waiting for him in his bedroom. It was all part of the rich tapestry of student life.
When Paul finished his degree he got a job with an accountancy firm to train as a chartered accountant. The office was in another town, where Paul moved, but he was still registered at the GP on campus. Whenever he had a GP appointment he would call into my lab so that we could go for a coffee. At that time it did not occur to me that it was odd how many times he was visiting his GP, but I later learned that for a while his immune system was compromised. Paul was very fit: he had been a county level cross country runner, was a keen cyclist and he did martial arts, so frequent trips to his GP was not normal.
Then early in January he turned up at my lab. Over coffee he said that he was about to see his GP because he had discovered some lumps in his armpit. It sounded worrying, so I asked him to call back after his appointment. On his return he told me that his GP was very worried about the lumps and said that he needed to see a cancer specialist at the University hospital just over the road. The problem was that this was 1988 and when she called the hospital she was told that there was a three month waiting list. Paul then asked her if his health insurance would help. At the end of December he had worked for the accountancy firm for six months and this meant that he was now part of the company's health insurance scheme. His GP told him it would, and called the hospital again. This time he was given an appointment for the same specialist the next day.
Then followed a whirlwind of activity. The specialist confirmed that it was cancer - a tumour in his neck - and two days later he was operated on to remove the tumour. Then he had months of chemo in a private hospital out in the country, and radiotherapy in a local NHS hospital. For his chemo his girlfriend would drive him to my house the night before, and we would have our own chemo session in the local pubs. The next day I would drive him to the hospital and a few days after his girlfriend would pick him up from the hospital to take him home.
As an accountant he cast a beady eye over the care he was getting. I don't know if he had requested a copy of the bill, or whether it was standard practice, but he took an interest in the cost of the drugs he was given. I remember him telling me how shocked he was over the huge levels of overcharging, but since it was being paid by the insurance company (and the premiums paid by his employer) he really didn't feel able to complain.
On one of these chemo sessions Paul took ill. It wasn't the usual nausea, it was far worse, so bad that the staff at the hospital called the specialist immediately. This was the same specialist who worked in the NHS hospital. I remember Paul telling me that the specialist turned up in a dinner suit - he had been bleeped while in the audience at the opera. It was a provincial theatre, so the opera must have been touring and hence the specialist was probably missing a performance that was unlikely to be repeated for a long time. Private patients were that special.
Then Paul needed an MRI scan. This was the early days of MRI. The technique had been developed fifteen doors down the corridor where I worked, but because it was a research lab they did not have the facilities for really sick patients. Instead, Paul was scanned in the University Hospital over the road. This hospital was one of five in the region that had clubbed together to buy their own MRI machine. It was installed in a container which was driven around the contributing hospitals on a regular schedule, spending a week or so in the car park of each one.
Paul described to me what happened. He was driven from the private hospital in a private ambulance. At the University Hospital he was put in a wheelchair and a porter took him to the queue of patients waiting to be scanned. Some sat on seats, some were in wheelchairs and others on trolleys. Paul was pushed past this queue of patients. He was pushed past this pitiful collection of humanity and pushed right to the front of the queue. I know that Paul had been grateful for his health insurance, because he had been told by the specialist that he may not have survived the NHS waiting list, but I knew from his voice when he told me about the MRI scan that he was truly ashamed of being pushed to the front of the queue. He could have waited but his status as a private patient meant that the other patients, regardless of how sick they were, did not count.
Paul recovered. He had two years of remission, and then the cancer returned. This time he was treated in an NHS hospital closer to his home. Although he still worked for the accountancy company, the health insurance no longer covered him. Sadly, his specialist could not determine the cause of the cancer. He had various operations to remove tumours from various parts of his body. Then it was discovered that he had a tumour between his spine and lungs. It was inoperable. But worse: the mineral balance in his blood was haywire and his lungs filled up with fluid which required a painful procedure to drain them.
By this time, I had changed jobs and moved house. My new job was unreasonably hectic, but luckily one weekend I did not have to work and so I visited Paul for the day. It was shocking. This once fit energetic man could barely move, and even the simplest of actions was difficult for him. I remember that the chairs in the sitting room had bricks under their legs: this was so that the seats were higher so that Paul could manage to get up after sitting down. He was too weak to get himself out of a armchair.
We spoke at length about his treatment, but his wife, a midwife, kept quiet. I later learned that she knew more about his condition than he did, she had asked the specialist the questions that he could not bring himself to ask.
The following weekend I phoned him to see how his treatment was progressing and he told me that his specialist had told him that his chemo had been stopped. I immediately recognised what was happening, but Paul was an eternal optimist. He told me about how there was an ultrasound technique that the hospital were trialling that could be used to drain the fluid from his chest. He told me about a new drug that he would be given once he had rested a while and regained his strength. He knew he had a future, I knew that he had been sent home to die.
The following Friday was my birthday. It was one of the few weeks that year that I was working in the office rather than on site. Mid morning I got a telephone call from my wife. She was tearful, she had had a phone call from the brother of Paul's wife (who, coincidentally, was the other student I had shared the house with). Paul had died that morning. He had drowned from the fluid in his lungs. The cancer had killed him.
I hated the job I was doing then. I felt bullied by my managers to work far longer hours than I was contracted to do and I felt that this company was making me neglect my family. When I found out when Paul's funeral was to be I told my manager - not requested, but told him - that I was going to the funeral. Paul was 28 when he died, in our modern age, and in peacetime, we do not expect people to die that young. I realised that life is too fragile and too short to allow others to exploit and abuse you. I changed jobs a month later.
Paul was never an advocate for private healthcare: during his years of remission he told me that his treatment had convinced him of the need for the NHS. It was partly the waste of the private hospital, the fact that they could charge whatever they wanted and the bill would be paid. This shocked Paul because it meant that they had no incentive to limit care to just what was needed. But I think his experience of being wheeled past the rows of NHS patients and taken to the front of the queue had a profound effect on him. I remember him describing the queue of people, and how he realised that the NHS treated everyone.
Now the days of Paul's treatment are returning. Thatcher's NHS was dire, but at least the service had real terms increases that could be counted in billions rather than Cameron's that can only be counted in millions and only then on a good day. Now patients are being denied NHS care: they are being told that they are not blind enough, or in enough pain to have the operation they need. Most of us thought that such days had been banished to the past, that the NHS existed to give us the care we needed, when we needed it. But now it is getting worse, we are seeing the return to the Thatcher doctrine that people should expect to pay for private care, either out of pocket or through insurance, and that those of us who could not afford private care would, like the queues of patients waiting for their MRI scan in that 80s hospital, be second in line to the private patients.
We are going back to the NHS of when Paul's cancer first appeared, but sadly, it can never bring back Paul.
When Paul finished his degree he got a job with an accountancy firm to train as a chartered accountant. The office was in another town, where Paul moved, but he was still registered at the GP on campus. Whenever he had a GP appointment he would call into my lab so that we could go for a coffee. At that time it did not occur to me that it was odd how many times he was visiting his GP, but I later learned that for a while his immune system was compromised. Paul was very fit: he had been a county level cross country runner, was a keen cyclist and he did martial arts, so frequent trips to his GP was not normal.
Then early in January he turned up at my lab. Over coffee he said that he was about to see his GP because he had discovered some lumps in his armpit. It sounded worrying, so I asked him to call back after his appointment. On his return he told me that his GP was very worried about the lumps and said that he needed to see a cancer specialist at the University hospital just over the road. The problem was that this was 1988 and when she called the hospital she was told that there was a three month waiting list. Paul then asked her if his health insurance would help. At the end of December he had worked for the accountancy firm for six months and this meant that he was now part of the company's health insurance scheme. His GP told him it would, and called the hospital again. This time he was given an appointment for the same specialist the next day.
Then followed a whirlwind of activity. The specialist confirmed that it was cancer - a tumour in his neck - and two days later he was operated on to remove the tumour. Then he had months of chemo in a private hospital out in the country, and radiotherapy in a local NHS hospital. For his chemo his girlfriend would drive him to my house the night before, and we would have our own chemo session in the local pubs. The next day I would drive him to the hospital and a few days after his girlfriend would pick him up from the hospital to take him home.
As an accountant he cast a beady eye over the care he was getting. I don't know if he had requested a copy of the bill, or whether it was standard practice, but he took an interest in the cost of the drugs he was given. I remember him telling me how shocked he was over the huge levels of overcharging, but since it was being paid by the insurance company (and the premiums paid by his employer) he really didn't feel able to complain.
On one of these chemo sessions Paul took ill. It wasn't the usual nausea, it was far worse, so bad that the staff at the hospital called the specialist immediately. This was the same specialist who worked in the NHS hospital. I remember Paul telling me that the specialist turned up in a dinner suit - he had been bleeped while in the audience at the opera. It was a provincial theatre, so the opera must have been touring and hence the specialist was probably missing a performance that was unlikely to be repeated for a long time. Private patients were that special.
Then Paul needed an MRI scan. This was the early days of MRI. The technique had been developed fifteen doors down the corridor where I worked, but because it was a research lab they did not have the facilities for really sick patients. Instead, Paul was scanned in the University Hospital over the road. This hospital was one of five in the region that had clubbed together to buy their own MRI machine. It was installed in a container which was driven around the contributing hospitals on a regular schedule, spending a week or so in the car park of each one.
Paul described to me what happened. He was driven from the private hospital in a private ambulance. At the University Hospital he was put in a wheelchair and a porter took him to the queue of patients waiting to be scanned. Some sat on seats, some were in wheelchairs and others on trolleys. Paul was pushed past this queue of patients. He was pushed past this pitiful collection of humanity and pushed right to the front of the queue. I know that Paul had been grateful for his health insurance, because he had been told by the specialist that he may not have survived the NHS waiting list, but I knew from his voice when he told me about the MRI scan that he was truly ashamed of being pushed to the front of the queue. He could have waited but his status as a private patient meant that the other patients, regardless of how sick they were, did not count.
Paul recovered. He had two years of remission, and then the cancer returned. This time he was treated in an NHS hospital closer to his home. Although he still worked for the accountancy company, the health insurance no longer covered him. Sadly, his specialist could not determine the cause of the cancer. He had various operations to remove tumours from various parts of his body. Then it was discovered that he had a tumour between his spine and lungs. It was inoperable. But worse: the mineral balance in his blood was haywire and his lungs filled up with fluid which required a painful procedure to drain them.
By this time, I had changed jobs and moved house. My new job was unreasonably hectic, but luckily one weekend I did not have to work and so I visited Paul for the day. It was shocking. This once fit energetic man could barely move, and even the simplest of actions was difficult for him. I remember that the chairs in the sitting room had bricks under their legs: this was so that the seats were higher so that Paul could manage to get up after sitting down. He was too weak to get himself out of a armchair.
We spoke at length about his treatment, but his wife, a midwife, kept quiet. I later learned that she knew more about his condition than he did, she had asked the specialist the questions that he could not bring himself to ask.
The following weekend I phoned him to see how his treatment was progressing and he told me that his specialist had told him that his chemo had been stopped. I immediately recognised what was happening, but Paul was an eternal optimist. He told me about how there was an ultrasound technique that the hospital were trialling that could be used to drain the fluid from his chest. He told me about a new drug that he would be given once he had rested a while and regained his strength. He knew he had a future, I knew that he had been sent home to die.
The following Friday was my birthday. It was one of the few weeks that year that I was working in the office rather than on site. Mid morning I got a telephone call from my wife. She was tearful, she had had a phone call from the brother of Paul's wife (who, coincidentally, was the other student I had shared the house with). Paul had died that morning. He had drowned from the fluid in his lungs. The cancer had killed him.
I hated the job I was doing then. I felt bullied by my managers to work far longer hours than I was contracted to do and I felt that this company was making me neglect my family. When I found out when Paul's funeral was to be I told my manager - not requested, but told him - that I was going to the funeral. Paul was 28 when he died, in our modern age, and in peacetime, we do not expect people to die that young. I realised that life is too fragile and too short to allow others to exploit and abuse you. I changed jobs a month later.
Paul was never an advocate for private healthcare: during his years of remission he told me that his treatment had convinced him of the need for the NHS. It was partly the waste of the private hospital, the fact that they could charge whatever they wanted and the bill would be paid. This shocked Paul because it meant that they had no incentive to limit care to just what was needed. But I think his experience of being wheeled past the rows of NHS patients and taken to the front of the queue had a profound effect on him. I remember him describing the queue of people, and how he realised that the NHS treated everyone.
Now the days of Paul's treatment are returning. Thatcher's NHS was dire, but at least the service had real terms increases that could be counted in billions rather than Cameron's that can only be counted in millions and only then on a good day. Now patients are being denied NHS care: they are being told that they are not blind enough, or in enough pain to have the operation they need. Most of us thought that such days had been banished to the past, that the NHS existed to give us the care we needed, when we needed it. But now it is getting worse, we are seeing the return to the Thatcher doctrine that people should expect to pay for private care, either out of pocket or through insurance, and that those of us who could not afford private care would, like the queues of patients waiting for their MRI scan in that 80s hospital, be second in line to the private patients.
We are going back to the NHS of when Paul's cancer first appeared, but sadly, it can never bring back Paul.
Wednesday 28 December 2011
A radical thought
OFT says that in 2008 the total market for private healthcare was estimated to be £5.5bn. They said that the NHS paid 23% of that or £1.3bn. Monitor says that in 2010 £252m of the income of Foundation Trusts (1.1%) was from private patients. It looks to me that so far private healthcare is "winning" by over a billion pounds per year.
So here's a radical thought. Rather than yet another upheaval in the vain attempt to try and get more of the leprechaun gold that is private patient income into NHS hospitals, why don't we just stop paying private hospitals to do NHS work? The NHS could do what it does well: cost effective, comprehensive, universal healthcare; the private sector can then do what it does: deep-pile carpet healthcare for people with leprechaun gold. And the NHS will be £1bn better off.
So here's a radical thought. Rather than yet another upheaval in the vain attempt to try and get more of the leprechaun gold that is private patient income into NHS hospitals, why don't we just stop paying private hospitals to do NHS work? The NHS could do what it does well: cost effective, comprehensive, universal healthcare; the private sector can then do what it does: deep-pile carpet healthcare for people with leprechaun gold. And the NHS will be £1bn better off.
Tuesday 27 December 2011
Private Patient Income Cap
The private patient income (PPI) cap was imposed to limit the private income of NHS trusts. The cap includes the income from actual physical, in-the-flesh, patients, but it also includes income from other services like providing pathology or income from intellectual property. This cap is arbitrary, Foundation Trusts are limited to the percentage of their income that came from private work in 2003. In 2010/11 FTs generated £252m income from private patients, this is 1.1% of their total income of £26,867m. There are, however, a few FTs that make considerably more than this (as I outlined in my post earlier this year):
The arbitrary nature of the PPI cap is unacceptable and needed fixing, but removing it entirely is not the solution. For a start, Intellectual Property should have been NHS IP and new techniques should have been used for all NHS patients, not just for those in the hospital that developed them. Then there is the fact that the cap does not distinguish between income from services provided by NHS hospitals for private hospitals and income from private patients. There is clearly a difference between the two, and I think that private patient numbers should be capped to prevent a two tier system, but the services should be regulated but excluded from the income cap.
The Times, apparently have a leak that says that the PPI cap will be raised to a maximum of 49%. I guess this is a "compromise" by Lansley to his Lib Dem opponents. The original policy in the White Paper (and in the Bill) was to abolish the cap completely. A "cap" of 49% will, frankly, have the same effect as abolishing the cap.
This leak has lead to some quite hysterical comments. The Independent, for example, reports:
It may be that the large London teaching hospitals (basically the hospitals listed above) will attract more foreign patients (but sufficient to get 49% of their income from private work?), but it is unlikely that your average bog standard district general hospital will be able to do that. In terms of private patients from England, the last few years has seen a fall in the number of people with private medical insurance (PMI), and a slight rise in the number of self-pay. Can it be possible that literally millions of people from England will choose to have private treatment in an NHS hospital either as self-pay or PMI? I mean, actually choose to pay?
Lansley says:
I have had discussions with governors at my local FT on this subject and the more naive Conservatives take Lansley's line. The majority of governors are more wary. Incidentally, my local FT was founded in the 1850s as a workhouse with an infirmary; the workhouse has closed and the infirmary (ie the hospital) has taken over the workhouse site. The current management offices occupy what remains of the original workhouse buildings, I am sure there is an allegory there... The infirmary treated the poor through charitable funds. The suggestion that private patients will fund NHS patients (the rich paying for the treatment of the poor) is not a million miles from the original founding principles of this hospital: is this what we want?
However, those governors who naively believe Lansley's statement seem to ignore the fact that private patients will not want to be treated with the hoi poloi, they will not want to have the same accommodation, nor be subject to the same waiting times, and all of this means that the trust will have to make the investment to provide a separate private patient unit so that the private patients will be kept separate from the great unwashed. Parking is a perennial problem at this Foundation Trust, and the relatives of private patients will not want to suffer the same problems that relatives of NHS patients do to obtain a parking place, so the hospital will have to provide a separate car park for them. Where will the capital for all this investment come from? We know that the large London teaching hospitals have been able to get such investment using their international (NHS-funded) reputation, but your average district general hospital won't. I know that my local DGH FT needs a new NHS eye clinic, so if they can find the money for a private patient unit with its own private car park, why can't they find the capital for an NHS clinic? When the conversation gets to this point governors make it clear to the hospital management that private patients are just too costly.
The second issue is that, as mentioned above, private medical insurers have found that in the last few years they are getting less business and consequently they are trying to squeeze their providers. For example, BUPA have recently de-listed BMI because the private hospital chain would not cut their rates. Under these circumstances would PMI accept that the private patient units in an NHS hospital deliberately subsidises NHS patients? Would self-pay patients be happy to learn that a proportion of the fee they are paying will pay for a patient to get the same care for free? I think not, and especially not if self-pay patients have been denied NHS care themselves (which will become increasingly the case in the next few years). This brings me to another issue.
The meme that is going round Twitter at the moment is that there are 160,000 beds in NHS hospitals and that if the PPI cap is raised to 49% 80,000 beds will be occupied by private patients. There are currently 11,200 beds in private acute hospitals at the moment, so even if all of those patients decided to go to a NHS hospital instead there would still be a shortfall of almost 70,000. This is not 70,000 per year, this is 70,000 at any one time, and represents a huge number of patients.
Where will all these new patients come from? This leads me to clause 10 of the Bill. This clause says that the responsibility of making the decision about charging for NHS treatment will be removed from the Secretary of State and it will be handed to Clinical Commissioning Groups. There will be about 250 of these, so it is likely that at least one will decide that the NHS will not pay for common treatments like cataracts, hips and knees. Further, the NHS cuts that is causing the impending NHS financial crisis will lead to Draconian rationing. CCGs will literally tell patients that they are not yet in enough pain for the NHS to pay for their hip operation, or they are not blind enough for a cataract operation. Such patients, understandably, will look to their savings, or will cash in a life insurance policy, or raid their pension fund, indeed anything to find the money to pay for the operation they desperately need.
These are the patients who will become private patients in NHS hospitals (since NHS private rates will be cheaper than the private hospitals). This is how the NHS will be privatised. The irony is that two years prior those patients would have had the same treatment for free, and this free-at-the-point-of-use principle would have been preserved if they had voted differently at the 2010 election.
| The Royal Marsden | 30.7% |
| Royal Brompton and Harefield | 14.4% |
| Moorfields Eye Hospital | 13.7% |
| University College London Hospitals | 6.6% |
| Papworth Hospital | 6.1% |
| Guy's & St Thomas' | 3.0% |
The arbitrary nature of the PPI cap is unacceptable and needed fixing, but removing it entirely is not the solution. For a start, Intellectual Property should have been NHS IP and new techniques should have been used for all NHS patients, not just for those in the hospital that developed them. Then there is the fact that the cap does not distinguish between income from services provided by NHS hospitals for private hospitals and income from private patients. There is clearly a difference between the two, and I think that private patient numbers should be capped to prevent a two tier system, but the services should be regulated but excluded from the income cap.
The Times, apparently have a leak that says that the PPI cap will be raised to a maximum of 49%. I guess this is a "compromise" by Lansley to his Lib Dem opponents. The original policy in the White Paper (and in the Bill) was to abolish the cap completely. A "cap" of 49% will, frankly, have the same effect as abolishing the cap.
This leak has lead to some quite hysterical comments. The Independent, for example, reports:
"It is expected to cause more friction within the coalition with a senior Liberal Democrat warning that it was part of an ideological drive that many in the party would oppose, the newspaper said. "without realising that the 49% figure was Baroness Williams' idea! (Again, I explain this in an earlier post.)
It may be that the large London teaching hospitals (basically the hospitals listed above) will attract more foreign patients (but sufficient to get 49% of their income from private work?), but it is unlikely that your average bog standard district general hospital will be able to do that. In terms of private patients from England, the last few years has seen a fall in the number of people with private medical insurance (PMI), and a slight rise in the number of self-pay. Can it be possible that literally millions of people from England will choose to have private treatment in an NHS hospital either as self-pay or PMI? I mean, actually choose to pay?
Lansley says:
which he knows to be nonsense.
"If these hospitals earn additional income from private work that means there will be more money available to invest in NHS services."
I have had discussions with governors at my local FT on this subject and the more naive Conservatives take Lansley's line. The majority of governors are more wary. Incidentally, my local FT was founded in the 1850s as a workhouse with an infirmary; the workhouse has closed and the infirmary (ie the hospital) has taken over the workhouse site. The current management offices occupy what remains of the original workhouse buildings, I am sure there is an allegory there... The infirmary treated the poor through charitable funds. The suggestion that private patients will fund NHS patients (the rich paying for the treatment of the poor) is not a million miles from the original founding principles of this hospital: is this what we want?
However, those governors who naively believe Lansley's statement seem to ignore the fact that private patients will not want to be treated with the hoi poloi, they will not want to have the same accommodation, nor be subject to the same waiting times, and all of this means that the trust will have to make the investment to provide a separate private patient unit so that the private patients will be kept separate from the great unwashed. Parking is a perennial problem at this Foundation Trust, and the relatives of private patients will not want to suffer the same problems that relatives of NHS patients do to obtain a parking place, so the hospital will have to provide a separate car park for them. Where will the capital for all this investment come from? We know that the large London teaching hospitals have been able to get such investment using their international (NHS-funded) reputation, but your average district general hospital won't. I know that my local DGH FT needs a new NHS eye clinic, so if they can find the money for a private patient unit with its own private car park, why can't they find the capital for an NHS clinic? When the conversation gets to this point governors make it clear to the hospital management that private patients are just too costly.
The second issue is that, as mentioned above, private medical insurers have found that in the last few years they are getting less business and consequently they are trying to squeeze their providers. For example, BUPA have recently de-listed BMI because the private hospital chain would not cut their rates. Under these circumstances would PMI accept that the private patient units in an NHS hospital deliberately subsidises NHS patients? Would self-pay patients be happy to learn that a proportion of the fee they are paying will pay for a patient to get the same care for free? I think not, and especially not if self-pay patients have been denied NHS care themselves (which will become increasingly the case in the next few years). This brings me to another issue.
The meme that is going round Twitter at the moment is that there are 160,000 beds in NHS hospitals and that if the PPI cap is raised to 49% 80,000 beds will be occupied by private patients. There are currently 11,200 beds in private acute hospitals at the moment, so even if all of those patients decided to go to a NHS hospital instead there would still be a shortfall of almost 70,000. This is not 70,000 per year, this is 70,000 at any one time, and represents a huge number of patients.
Where will all these new patients come from? This leads me to clause 10 of the Bill. This clause says that the responsibility of making the decision about charging for NHS treatment will be removed from the Secretary of State and it will be handed to Clinical Commissioning Groups. There will be about 250 of these, so it is likely that at least one will decide that the NHS will not pay for common treatments like cataracts, hips and knees. Further, the NHS cuts that is causing the impending NHS financial crisis will lead to Draconian rationing. CCGs will literally tell patients that they are not yet in enough pain for the NHS to pay for their hip operation, or they are not blind enough for a cataract operation. Such patients, understandably, will look to their savings, or will cash in a life insurance policy, or raid their pension fund, indeed anything to find the money to pay for the operation they desperately need.
These are the patients who will become private patients in NHS hospitals (since NHS private rates will be cheaper than the private hospitals). This is how the NHS will be privatised. The irony is that two years prior those patients would have had the same treatment for free, and this free-at-the-point-of-use principle would have been preserved if they had voted differently at the 2010 election.
Thursday 15 December 2011
Are you afraid of the facts?
Joe Farrington-Douglas pointed out on Twitter Lord Owen's speech, on Tuesday, about compettition and Monitor. This section is interesting:
In 2006, a Labour Government commissioned a major study on competition and the effects on the EU. It is a scandal that I have been trying for months through Freedom of Information to get hold of this document so that we would have it before this debate.Why can't we have this report? And could Patricia Hewitt, who was Secretary of State at the time, tell us what the report said?
I have been obstructed at every turn by the Department of Health. Do not tell me that it wants the facts out here so that we can discuss them and know about this issue. As the noble Lord [Howe] states, as an experienced lawyer, this is an area of very great complexity and yet we are not allowed to see this study, which we have paid for. It is not the possession of the Government-it was not even commissioned by this Government-but we are not allowed to see it. What is the Freedom of Information Act about? Are you afraid of the facts? Is there something that we cannot be trusted with? We are about to legislate on a very important area, which does have an impact on the EU, and we are deprived of one of the existing studies. So, all of us have had to go around and try to get expertise in this area and it is not easy to do so.
Wednesday 14 December 2011
Lady Williams
This is an interesting quote from a forthcoming interview with Andrew Lansley in the Spectator about Shirley Williams. (Quoted on the Guardian website):
When asked what he makes of her, the Health Secretary is lost for words. 'She is...' he splutters. 'How can I say, she is... a high maintenance date. We have had lots of meetings,' he continues. 'In a sense, to give her her due, even if I felt we had to devote an enormous amount of time simply to get to the point where we were clear about what it is she wanted, I think that allowed her to realise that we were not dealing with the bill as she imagined it was.'Lady Williams is the Lib Dems' great hope for the Health Bill in the Lords. In this respect I agree with Lansley, Lady Williams does not appear to understand the Bill.
Diabetes Audit
There is something a bit odd about the shock news released today that people who have a serious (but controllable) medical condition are not expected to live as long as people without it. As per usual, the BBC are reporting the news as if no one has ever been aware of it, but I came to the conclusion a year ago that the BBC have an agenda to broadcast as many articles as possible that puts the NHS in a poor light. (Not surprising really, since that is the agenda of the Department of Health and the BBC seems to be the biggest consumer of churnalism at the moment.)
Let's look at what the BBC are saying.
ONS says that in 2010 there were 493,000 deaths in the UK. Out of a population of 62 million that means slightly under 0.8% of the population. ONS provides detailed tables giving the cause of death.

The figures says that in 2010, 5,223 people died from diabetes. When just over five thousand people die from diabetes a year, the BBC says that almost five times more deaths can be avoided. How? Perhaps this statement from the BBC article explains why:
The BBC says:
Then the BBC report this:
Eh? They have known since 2004 that there were shocking variations and have done nothing about it? Are the Department of Health that incompetent?
The BBC report is churnalism of the press release on the NHS Information Centre. The news is not shocking, it is well known, the NHS IC merely have produced a report about something we all knew anyway. Perhaps the most interesting part of the NHS IC report is this:
Let's look at what the BBC are saying.
"Up to 24,000 deaths from diabetes could be avoided in England each year, if patients and doctors better managed the condition, a report concludes."Let's look at the statistics. Diabetes UK say that there are 2.9 million people with diabetes (type 1 and type 2) or 4.45% of the UK population. They also say that 90% of diabetics have type 2 diabetes.
ONS says that in 2010 there were 493,000 deaths in the UK. Out of a population of 62 million that means slightly under 0.8% of the population. ONS provides detailed tables giving the cause of death.

The figures says that in 2010, 5,223 people died from diabetes. When just over five thousand people die from diabetes a year, the BBC says that almost five times more deaths can be avoided. How? Perhaps this statement from the BBC article explains why:
"Around 70-75,000 diabetic patients die every year."This is not the number of people who die from diabetes, this is the number of diabetics who die. Such people could be dying of cancer, stroke or heart attacks; in other words the same things that everyone else dies of. Diabetes may well exasperate these conditions, but that is not the same as dying from diabetes; ONS says so.
The BBC says:
For patients with Type 1, the risk of dying was 2.6 times higher than it was for the general population. With Type 2, the risk was 1.6 times higher.The figures that I gave above from Diabetes UK about diabetes mortality are also in a PDF report on their website called Diabetes in the UK 2010: Key statistics on diabetes. In a section called Life expectancy and mortality it has these statistics:
More than one in ten (11.6 per cent) deaths among 20 to 79-year-olds in England can be attributed to diabetes. If current trends continue, one in eight (12.2 per cent) deaths among 20 to 79-year-olds will be attributable to the condition by 2010.Note the date: 2010. In fact, the figures for the reduction in life expectancy comes from a Department of Health report dated 2001. The 11.6% figure comes from a report in 2008. In other words, none of this is new.
Life expectancy is reduced, on average, by:
– more than 20 years in people with Type 1 diabetes
– up to 10 years in people with Type 2 diabetes
Then the BBC report this:
The Department of Health in England said shocking variations in care and an unacceptable death toll were evident.Where did they get this impression from? Variation in the treatment of diabetes can be obtained from the Quality Outcomes Framework, that the Department of Health have been collecting since 2004.
Eh? They have known since 2004 that there were shocking variations and have done nothing about it? Are the Department of Health that incompetent?
The BBC report is churnalism of the press release on the NHS Information Centre. The news is not shocking, it is well known, the NHS IC merely have produced a report about something we all knew anyway. Perhaps the most interesting part of the NHS IC report is this:
"There is a strong link between deprivation and increased mortality rates. Among under-65s with diabetes; the number of deaths among people from the most deprived backgrounds is double that of those from the least deprived backgrounds."This re-states something that was in the Diabetes Audit (pdf) from last year:
"In those aged 70 years and over, similar numbers of Q1 (12.1 per cent) and Q5 (14.8 per cent) have Type 2 diabetes, but under the age of 55 Type 2 diabetes is more than twice as common in Q5 (3.0 per cent) as Q1 (1.3 per cent). This may reflect lifestyle differences in exercise, diet and weight."Q1 is the least deprived quintile of the population, Q5 is the most deprived. There is a clear message here: deprivation causes type 2 diabetes. The BBC didn't report that, did they?
Tuesday 13 December 2011
NHS Funding
Two interesting bits of information have come out over the last couple of days. The first is from an interview by James Forsyth with Andrew Lansley in the Spectator:
The problem is that at the Autumn Spending Review George Osborne admitted to his mismanagement of the economy and, shamefaced, accepted that his plan to wipe out the structural deficit will be delayed by two years. So rather than getting a balanced budget by the next election, the balance will be achieved two years later. If the economy is in such a Tory-imposed mess, how can Lansley promise "real term increases"?
The clue lies in an article by Nick Timmins of the FT. The title of the article tells you almost all you need to know: Debate looms about how to fund the NHS. In this Timmins says:
[As an aside, if there is an NHS financial crisis before the next election then surely the public will take this to finally decide that the NHS is not safe in Tory hands? If so then we have to direct our attention to Labour and get a pledge from them to maintain the current funding mechanism.]
When have we heard this before? We haven't had such an option specifically at an election (there's always a first time). However, after the Blair government introduced tuition fees (without an electoral mandate) we were told that we had to accept the new funding mechanism because it was the only way to provide the extra funding that higher education needed. Same argument, different public service.
We know that the introduction of tuition fees was a disaster, contributing to the heavy debts our children will have to bear. Let's hope that the next time that a political party either seeking a mandate, or in power without the mandate, will find all-out opposition to the funding changes that Timmins suggests could be offered.
'I ask him whether, despite the ramifications of the autumn statement, the NHS budget will still be immune from cuts. His reply is unequivocal: "We have been very clear that the NHS is going to have real terms increases year on year. I mean clearly what we've said in terms of the coalition agreement is an agreement for a parliament. From our point of view, I would say yes is the answer to that because exactly the same principles apply. We have a profile of rising demographics and demand and cost pressures and technology in the NHS, so it is inconceivable that we can sustain the quality of services that we are looking for without the basis of real terms increases."
Does this mean that spending on the NHS will have to rise in real terms every year from now until kingdom come? "I believe so."'Lansley is saying that a Tory government will not cut the NHS budget (as we know, their definition of real terms increase is actually real terms flat funding, but at least that is better than real terms cuts). This raises the question of whether Lansley is making up policy? Forsyth goes on:
'One senior figure at No. 10 tells me that "Dave, George and Steve", the holy trinity of Cameron, Osborne and Hilton, "all believe that the pressures on the Health Service are such that you are always going to have to increase spending on it"'.So it seems that "real terms increases" after the election is a Tory policy. It is questionable whether it will be enough to de-toxify the Tory brand on the NHS after Lansley's mismanagement, but that is another article.
The problem is that at the Autumn Spending Review George Osborne admitted to his mismanagement of the economy and, shamefaced, accepted that his plan to wipe out the structural deficit will be delayed by two years. So rather than getting a balanced budget by the next election, the balance will be achieved two years later. If the economy is in such a Tory-imposed mess, how can Lansley promise "real term increases"?
The clue lies in an article by Nick Timmins of the FT. The title of the article tells you almost all you need to know: Debate looms about how to fund the NHS. In this Timmins says:
"Last month’s autumn statement has made that more or less inevitable. Faced with rising demand, the health service was already facing its toughest financial challenge – four years of what is, in effect, a real terms freeze. But the extra £15bn a year of spending cuts beyond 2015 announced by the chancellor means that – unless the economy improves – the service will be in a financial crisis or on the brink of one."This is not the rosy situation that Lansley et al like to convey. Timmins is a reliable and expert social commentator: he knows his stuff. The NHS will suffer from a financial crisis at the next election and the Tory government will not be able to fund it sufficiently to fix the problem. Timmins describes what he thinks will happen:
"So when yet more money is excised from public services after the next election, it is inconceivable that the NHS will be given even the relative degree of protection it has received this time round. The result is likely to be a performance and financial crisis. Every time that has happened – in the 1980s, 1990s and early 2000s – the result has been a debate about how to fund the service, with all the old chestnuts dragged out. Whether, for example, to introduce charges, provide tax relief for private medical cover or switch to social insurance. Up to now, such arguments have always been lost. This time round, the outcome may be different, not least because other forces are at work."While I do not think that Osborne deliberately engineered a failing economy so as to create an excuse for this debate, I do think that it was the intention of his policy of real terms flat funding. At the next election the Tories will go to the country telling the electorate that the only way for the NHS to have the larger increases necessary to avert the financial crisis is if the electorate accepts a new funding mechanism.
[As an aside, if there is an NHS financial crisis before the next election then surely the public will take this to finally decide that the NHS is not safe in Tory hands? If so then we have to direct our attention to Labour and get a pledge from them to maintain the current funding mechanism.]
When have we heard this before? We haven't had such an option specifically at an election (there's always a first time). However, after the Blair government introduced tuition fees (without an electoral mandate) we were told that we had to accept the new funding mechanism because it was the only way to provide the extra funding that higher education needed. Same argument, different public service.
We know that the introduction of tuition fees was a disaster, contributing to the heavy debts our children will have to bear. Let's hope that the next time that a political party either seeking a mandate, or in power without the mandate, will find all-out opposition to the funding changes that Timmins suggests could be offered.
Monday 5 December 2011
Data
There is nothing new about the collection of medical data. The industrial revolution had a huge effect on the lives of many people, particularly the poor, but it was the Boer War that brought public health to the forefront. The military found that a large proportion of recruits for the war were unfit for service. Although there were philanthropic health visitors before then, the scandal of the Boer War was the impetus to expand the service. By the end of the First World War there were more than 3,000 health visitors with a specific mandate to work with mothers and promote infant and child care and the prevention of the spread of infection. The Victorians were enamoured with figures, and health visitors, of course, could record lots of figures. A century of data of child development is valuable for people researching the subject.
When you look at data, you can look at it from one end of the telescope or the other. Holding the telescope normally, you can get detailed information about an individual. If you access health records from the early part of the 20th century you could get information about people who are still alive. Such data may be so detailed as to make it personal, but such information will have little importance other than to the individual. If you turn the telescope around and look at aggregated data, you get a much bigger picture, one which allows you to make decisions about large groups of people. However, since detail is a hindrance aggregated data means that the individual cannot be seen.
The announcement that the government intends to hand our medical records over to private companies worries some people because they feel their privacy will be invaded. Can you say that the data that the health visitors gathered a century ago was an invasion of the privacy of those children? In response to the government's plans to hand NHS data to private companies the campaign group Patient Concern said:
However, as I explained in my last blog, it depends on how you interpret the data. For example, a friend was an administrator in the transplant unit of a large hospital. At that time George Best needed a new liver. My friend told me that in his hospital a young person died. This person had indicated that they wanted to donate their organs and their family had agreed too. The person was an appropriate tissue match for Best, but the family were not told this because donations are anonymous, however, they were told that the young person's liver had been transplanted. This tiny piece of information was significant because a few hours later the media reported that Best had received a new liver. The family could easily put two and two together, and (so my friend told me) were upset that their child's liver would be transplanted into someone who would abuse it (as proved to be the case).
A small piece of information - the organ that had been transplanted - allowed the family to find out who had received the organ. While it is possible to anonymise a process, or to anonymise data, it has to be done carefully, particularly when you are handing a single patient's anonymised data. This does not mean that anonymised data can "easily be re-identified" but it does mean that sometimes people can make intelligent guesses. When data is aggregated even more detail is lost, and even the most intelligent cannot make guesses about the individuals involved.
UPDATE:
@NO2ID tweeted this article from the security guru, Bruce Schneier (if you have the chance, read Schneier's "Beyond Fear"). In the article he reports studies that have essentially used external data to make "intelligent guesses" with online databases.
When you look at data, you can look at it from one end of the telescope or the other. Holding the telescope normally, you can get detailed information about an individual. If you access health records from the early part of the 20th century you could get information about people who are still alive. Such data may be so detailed as to make it personal, but such information will have little importance other than to the individual. If you turn the telescope around and look at aggregated data, you get a much bigger picture, one which allows you to make decisions about large groups of people. However, since detail is a hindrance aggregated data means that the individual cannot be seen.
The announcement that the government intends to hand our medical records over to private companies worries some people because they feel their privacy will be invaded. Can you say that the data that the health visitors gathered a century ago was an invasion of the privacy of those children? In response to the government's plans to hand NHS data to private companies the campaign group Patient Concern said:
'This is the death of patient confidentiality. There is no guarantee that information will be anonymised. In any case, anonymised data can just as easily be re-identified.'This is nonsense. Anonoymising data is one-way: once you have removed identifying data there is no way that someone else can put it back in. The suggestion from Patient Concern is as believable as homoeopaths claiming that water has "memory", the campaign group seems to be suggesting that patient data has "memory".
However, as I explained in my last blog, it depends on how you interpret the data. For example, a friend was an administrator in the transplant unit of a large hospital. At that time George Best needed a new liver. My friend told me that in his hospital a young person died. This person had indicated that they wanted to donate their organs and their family had agreed too. The person was an appropriate tissue match for Best, but the family were not told this because donations are anonymous, however, they were told that the young person's liver had been transplanted. This tiny piece of information was significant because a few hours later the media reported that Best had received a new liver. The family could easily put two and two together, and (so my friend told me) were upset that their child's liver would be transplanted into someone who would abuse it (as proved to be the case).
A small piece of information - the organ that had been transplanted - allowed the family to find out who had received the organ. While it is possible to anonymise a process, or to anonymise data, it has to be done carefully, particularly when you are handing a single patient's anonymised data. This does not mean that anonymised data can "easily be re-identified" but it does mean that sometimes people can make intelligent guesses. When data is aggregated even more detail is lost, and even the most intelligent cannot make guesses about the individuals involved.
UPDATE:
@NO2ID tweeted this article from the security guru, Bruce Schneier (if you have the chance, read Schneier's "Beyond Fear"). In the article he reports studies that have essentially used external data to make "intelligent guesses" with online databases.
Anonymising Data
Today we hear that The Prime Minister wants to sell off NHS data (sorry, "he wants to make it easier for drug companies to run clinical trials in hospitals and to benefit from the NHS's vast collection of patient data"). This has prompted much howling from people scared that private companies will have access to their medical records. This is not the case (although Lansley wants you to voluntarily hand over your full medical records to private companies, but that is another policy yet to be debated).
It is easy to provide rich, anonymised data: simply remove your name and address. However, this removes important data since your location may be affecting your health. Researchers trying to use the data to look for connections between health and the various factors given in the dataset need to take into account any variations due to location. There are 28 million addresses in the UK. Your postcode covers about 15 addresses, so the combination of your house number and postcode identifies your home.
Your postcode comes in two parts. The first part is called the Outward Code, and the second part is the Inward Code. Each of these can be split into two. The postcode PO1 2AF can be split like this (this is data from the Post Office's lengthy document on postcodes and I have assumed total population is 60 million):
The point of this table is that it shows that by giving some of the postcode you can make the data more localised, while anonymising the data. If the entire postcode is provided then there is a good change the patient can be identified. However, such data would be too granular to be useful for data mining anyway. Data grouped by Postcode Sector (giving 11,000 unique locations) or Postcode District (giving about 3,000 unique locations) is much more manageable.
Let's imagine that that a celebrity actress has just had an operation on her foot and is on crutches. She has recently been on Strictly Come Dancing so the tabloid paparazzi think it is newsworthy to have a picture of her on crutches. The paps obtain a spreadsheet of all the people who have had foot operations in the last month. If the spreadsheet has the actress's house number and postcode, they can can simply park outside her house and take pictures of anything that moves within. If they have just her postcode, they have a one in fifteen chance of getting the right address and most likely will knock on one door in that postcode area and ask which house the actress lives in - eventually they find out the right house.
If the data has the Postcode Sector, it means that it covers 2,500 addresses (or about 5,400 people). It is not feasible for the pap to visit all the streets in the Postcode Sector on the random chance that they may be able to see an actress on crutches. However, 5,400 people is around the size of the patient list of a GP practice, so if the paparazzi loiter by the GP practice that covers that area they are bound to be able to take pictures of someone on crutches with a bandaged foot. There is a chance that the patient will be the actress. The more "innovative" paps will realise that from the Postcode Sector they can identify the community health team, the paps can then find out who the physiotherapists are and try to extract the address from them. Incidentally, the Postcode Sector is also roughly the size of an electoral ward (there is a large variation of the population size of electoral wards across the country).
For location information to be useful for epidemiologically it needs some granularity, and the larger the area, the less useful the location data will be. If the data has the Postcode District this will cover about 20,000 people (9,400 addresses), which is a small town. Since there are 250 NHS Trusts (and about 500 hospitals) in England the PostCode District will identify the hospital where the operation was carried out (and most likely where follow up outpatients will be). The paps could wait outside outpatients on the day that the follow ups for foot operations are booked and hope the actress turns up. If the data has just the Postcode Area, then the paps cannot even identify the trust since there would be two, or (in cities) more trusts covering that area. However, it is likely that such data would have the trust identifying code, or the hospital identifying code.
The privacy concerns about NHS data being handed to private companies are unfounded. It is easy to anonymise data while still providing enough granularity. However, this is not my complaint against Cameron's decision. I will explain why I am not in favour of this policy in my next blog.
It is easy to provide rich, anonymised data: simply remove your name and address. However, this removes important data since your location may be affecting your health. Researchers trying to use the data to look for connections between health and the various factors given in the dataset need to take into account any variations due to location. There are 28 million addresses in the UK. Your postcode covers about 15 addresses, so the combination of your house number and postcode identifies your home.
Your postcode comes in two parts. The first part is called the Outward Code, and the second part is the Inward Code. Each of these can be split into two. The postcode PO1 2AF can be split like this (this is data from the Post Office's lengthy document on postcodes and I have assumed total population is 60 million):
| Outward Code | Inward Code | |||
| PostCode Area | Postcode District | Postcode Sector | Unit Postcode | |
| Postcode | PO | 1 | 2 | AF |
| Number of areas | 124 | 2,980 | 11,159 | 1.8 million |
| Addresses | 226,000 | 9,400 | 2,500 | 15 |
| People | 484,000 | 20,000 | 5,400 | 33 |
The point of this table is that it shows that by giving some of the postcode you can make the data more localised, while anonymising the data. If the entire postcode is provided then there is a good change the patient can be identified. However, such data would be too granular to be useful for data mining anyway. Data grouped by Postcode Sector (giving 11,000 unique locations) or Postcode District (giving about 3,000 unique locations) is much more manageable.
Let's imagine that that a celebrity actress has just had an operation on her foot and is on crutches. She has recently been on Strictly Come Dancing so the tabloid paparazzi think it is newsworthy to have a picture of her on crutches. The paps obtain a spreadsheet of all the people who have had foot operations in the last month. If the spreadsheet has the actress's house number and postcode, they can can simply park outside her house and take pictures of anything that moves within. If they have just her postcode, they have a one in fifteen chance of getting the right address and most likely will knock on one door in that postcode area and ask which house the actress lives in - eventually they find out the right house.
If the data has the Postcode Sector, it means that it covers 2,500 addresses (or about 5,400 people). It is not feasible for the pap to visit all the streets in the Postcode Sector on the random chance that they may be able to see an actress on crutches. However, 5,400 people is around the size of the patient list of a GP practice, so if the paparazzi loiter by the GP practice that covers that area they are bound to be able to take pictures of someone on crutches with a bandaged foot. There is a chance that the patient will be the actress. The more "innovative" paps will realise that from the Postcode Sector they can identify the community health team, the paps can then find out who the physiotherapists are and try to extract the address from them. Incidentally, the Postcode Sector is also roughly the size of an electoral ward (there is a large variation of the population size of electoral wards across the country).
For location information to be useful for epidemiologically it needs some granularity, and the larger the area, the less useful the location data will be. If the data has the Postcode District this will cover about 20,000 people (9,400 addresses), which is a small town. Since there are 250 NHS Trusts (and about 500 hospitals) in England the PostCode District will identify the hospital where the operation was carried out (and most likely where follow up outpatients will be). The paps could wait outside outpatients on the day that the follow ups for foot operations are booked and hope the actress turns up. If the data has just the Postcode Area, then the paps cannot even identify the trust since there would be two, or (in cities) more trusts covering that area. However, it is likely that such data would have the trust identifying code, or the hospital identifying code.
The privacy concerns about NHS data being handed to private companies are unfounded. It is easy to anonymise data while still providing enough granularity. However, this is not my complaint against Cameron's decision. I will explain why I am not in favour of this policy in my next blog.
Saturday 3 December 2011
TUPE
Transfer of Undertakings (Protection of Employment) regulations, or TUPE, was introduced by the last government to protect workers rights when they are transferred to another organisation (the law is the UK's implementation of a European directive). TUPE is on many people's lips now because the current government wants to divest itself of as much of its public service responsibilities as it can by shifting services into the so-called "voluntary sector" (social enterprises - not-for-profit private companies) or the private sector. To a large extent, the government does not care whether the public service is moved to the private sector or becomes a social enterprise, their only criteria is that the service should no longer be provided by the public sector.
When a service moves out of the public sector employees are rightly worried. After all, such employees signed a contract when they started the job and employment contracts are two way - the employer must keep to their contractual terms. TUPE attempts to ensure that the employee's terms and conditions are preserved even though the employer has changed. However, it is not all rosy. TUPE does not mean that an employee will still be able to contribute to the NHS pension scheme, the regulations merely says that the new employer must provide an equivalent scheme. And TUPE only affects existing employees, so new employees will be employed on different T&Cs (a two-tier system) and TUPEd staff changing roles within the new organisation will lose their TUPEd rights when they sign a new employment contract.
In the Autumn Statement, the government indicated that they wanted to change TUPE. The Chancellor said that this was to "help employers to hire people". There is some logic to this: making a profit from the NHS tariff is difficult enough, but it is made more difficult when an employer has to give their staff decent terms and conditions. Remove the requirement to pay staff a liveable income and it starts to get more attractive for the private sector to take over NHS services. If TUPE is abolished or watered down, it will mean worse conditions for staff: lower pay, loss of rights to training and loss of rights to a proper pension scheme.
However, TUPE is not just about transfers from the public to the private sector, it is about all transfers: within the private sector and within the public sector. So if a Foundation Trust (part of the NHS) takes over the Community Health Services from the local Primary Care Trust (part of the NHS), the employees are TUPEd. The transfer is within the NHS, but the regulations still apply. This is important because, nominally, FTs can employ staff on local terms and pay. At the moment only Southend Foundation Trust has used these "freedoms" to opt out of Agenda For Change and recently chose not to award annual increments that have resulted elsewhere under A4C.
TUPE effectively keeps T&Cs constant across the NHS. If TUPE were to be abolished this would quite rapidly result in local T&Cs and the first casualty will be Agenda For Change. Why not have local pay bargaining, after all, it costs far more to live in London than it does to live in Middlesbrough, so why not pay London workers more to reflect this? This happens already, NHS pay has a London-weighting. The problem with local pay is inherent in the name. It is not so much the difference between trusts in different parts of the country, it is the difference between trusts in the same part of the country. If there are two trusts in a city they can use local pay to compete for staff. If one trust pays more to attract more skilled staff, the effect will be that the trust that cannot pay the higher rates will not get the skilled staff. The result will be self-fulfilling: pay escalation for some staff and trusts that cannot afford the rates will have declining quality, declining patient numbers, declining income and then, ultimately, bankruptcy.
The real reason for wanting to abolish TUPE is that the government wants to move away from national pay bargaining and move to local T&Cs. The NHS works because it is one organisation. Fragmentation through different T&Cs and local pay bargaining will mark the end of the NHS since it will be the death of collaboration between NHS organisations.
When a service moves out of the public sector employees are rightly worried. After all, such employees signed a contract when they started the job and employment contracts are two way - the employer must keep to their contractual terms. TUPE attempts to ensure that the employee's terms and conditions are preserved even though the employer has changed. However, it is not all rosy. TUPE does not mean that an employee will still be able to contribute to the NHS pension scheme, the regulations merely says that the new employer must provide an equivalent scheme. And TUPE only affects existing employees, so new employees will be employed on different T&Cs (a two-tier system) and TUPEd staff changing roles within the new organisation will lose their TUPEd rights when they sign a new employment contract.
In the Autumn Statement, the government indicated that they wanted to change TUPE. The Chancellor said that this was to "help employers to hire people". There is some logic to this: making a profit from the NHS tariff is difficult enough, but it is made more difficult when an employer has to give their staff decent terms and conditions. Remove the requirement to pay staff a liveable income and it starts to get more attractive for the private sector to take over NHS services. If TUPE is abolished or watered down, it will mean worse conditions for staff: lower pay, loss of rights to training and loss of rights to a proper pension scheme.
However, TUPE is not just about transfers from the public to the private sector, it is about all transfers: within the private sector and within the public sector. So if a Foundation Trust (part of the NHS) takes over the Community Health Services from the local Primary Care Trust (part of the NHS), the employees are TUPEd. The transfer is within the NHS, but the regulations still apply. This is important because, nominally, FTs can employ staff on local terms and pay. At the moment only Southend Foundation Trust has used these "freedoms" to opt out of Agenda For Change and recently chose not to award annual increments that have resulted elsewhere under A4C.
TUPE effectively keeps T&Cs constant across the NHS. If TUPE were to be abolished this would quite rapidly result in local T&Cs and the first casualty will be Agenda For Change. Why not have local pay bargaining, after all, it costs far more to live in London than it does to live in Middlesbrough, so why not pay London workers more to reflect this? This happens already, NHS pay has a London-weighting. The problem with local pay is inherent in the name. It is not so much the difference between trusts in different parts of the country, it is the difference between trusts in the same part of the country. If there are two trusts in a city they can use local pay to compete for staff. If one trust pays more to attract more skilled staff, the effect will be that the trust that cannot pay the higher rates will not get the skilled staff. The result will be self-fulfilling: pay escalation for some staff and trusts that cannot afford the rates will have declining quality, declining patient numbers, declining income and then, ultimately, bankruptcy.
The real reason for wanting to abolish TUPE is that the government wants to move away from national pay bargaining and move to local T&Cs. The NHS works because it is one organisation. Fragmentation through different T&Cs and local pay bargaining will mark the end of the NHS since it will be the death of collaboration between NHS organisations.
Thursday 24 November 2011
Not in my name
The government is very keen on using people with long term conditions as an excuse for their changes to the NHS. They say that without the changes we will use so much healthcare that we will bankrupt the NHS. I am not against change, but I am against blaming people for unpopular change.
On the 18 January 1976, at the age of 11, I was diagnosed with type 1 diabetes. I remember, during one of the appointments I had with the diabetes specialist, I was told that in later life I would have kidney problems; there was no "if", it was a definite statement based on the middle aged diabetics that he was treating at that time. I distinctly remember the specialist telling me that by the time I am 50 I will need a new kidney.
A lot has changed since then. I am three years off the half century and my kidneys are still working. Part of the reason for this is because of the preventative medication I have been taking for the last 15 years or so (ACE inhibitors and calcium channel blockers for hypertension). Part of this is because of better management of my condition through purer insulin and through finger prick blood tests. None of this costs much, in fact through new processes of making insulin the price of insulin has dropped over the last 30 years. It is cheap to keep me alive!
Dialysis, organ transplant and the long term follow up care for a patient with a transplanted organ is expensive. In 1976 a health economist could have looked at me and visualised a deep pit being dug to consume future piles of NHS money. The health economist would have been wrong. I am sure that I have cost the NHS a lot less than could have been predicted 35 years ago.
I am going to be uncharacteristically optimistic here: I do not think I will be a big drain on NHS finances in the future either. This is why I wish the government will stop using me as their reason for breaking apart the NHS.
On the 18 January 1976, at the age of 11, I was diagnosed with type 1 diabetes. I remember, during one of the appointments I had with the diabetes specialist, I was told that in later life I would have kidney problems; there was no "if", it was a definite statement based on the middle aged diabetics that he was treating at that time. I distinctly remember the specialist telling me that by the time I am 50 I will need a new kidney.
A lot has changed since then. I am three years off the half century and my kidneys are still working. Part of the reason for this is because of the preventative medication I have been taking for the last 15 years or so (ACE inhibitors and calcium channel blockers for hypertension). Part of this is because of better management of my condition through purer insulin and through finger prick blood tests. None of this costs much, in fact through new processes of making insulin the price of insulin has dropped over the last 30 years. It is cheap to keep me alive!
Dialysis, organ transplant and the long term follow up care for a patient with a transplanted organ is expensive. In 1976 a health economist could have looked at me and visualised a deep pit being dug to consume future piles of NHS money. The health economist would have been wrong. I am sure that I have cost the NHS a lot less than could have been predicted 35 years ago.
I am going to be uncharacteristically optimistic here: I do not think I will be a big drain on NHS finances in the future either. This is why I wish the government will stop using me as their reason for breaking apart the NHS.
Sunday 13 November 2011
What's happening in the Lords
Yesterday I attended Labour's West Midlands Regional Conference. The day was dominated by a debate on the economy and workshops on developing policy. Notably absent was any session on the NHS: Labour are very quiet about what their policy will be, whether this is embarrassment because they handed the Tories a legislative framework that would enable them to marketise the NHS is unclear.
Anyway, in the final Q&A session, in response to a question on the NHS (just one!) Lord Hunt mentioned the changed voting habits of the upper house. Michael White mentions this too, in the Guardian:
The Bill sailed through the Commons Committee stage precisely because the Lib Dem members voted en bloc with the Tories. Not one single Labour amendment was passed by the Commons Committee. In fact not one single non-Government amendment was passed, because the Tory whips threatened Tory and Lib Dem MPs telling them that the only amendments that would be allowed to pass the Commons Committee would be those proposed by the government. This is the behaviour of a authoritarian government that believes that it is always right (a very frightening concept). We are finding the same behaviour in the Lords Committee.
If the Tories had not been handed a Coalition, and were now ruling by supply and confidence, the Lib Dem peers would be free to make amendments and make this bill better. Even if the Tories had scraped through the 2010 with a narrow majority, the Lib Dem peers would more often than not be changing this bill. Now they are sitting on their hands. It is very clear: Coalition is bad, and allows bad laws to pass.
Anyway, in the final Q&A session, in response to a question on the NHS (just one!) Lord Hunt mentioned the changed voting habits of the upper house. Michael White mentions this too, in the Guardian:
"When Labour was in power, the party's chief whip Lord Bassam could expect to lose one in three divisions if the Lib Dem, Tory and crossbench peers decided to strike down an offending clause in legislation. On issues like 42-day detention of terror suspects, defeated by the Lords in 2008, the unelected house spoke for public opinion. David Cameron's rose garden pact with Nick Clegg has changed the maths. With 170 Tory and 88 Lib Dem peers (the 153 crossbenchers often split 50/50) the coalition partners usually have a de facto majority over Labour's 238. No one party was supposed to have one in the half-reformed system bequeathed by Tony Blair, but no one planned for coalition. Government defeats are down to around 15%."Yet again, the Lib Dems are allowing this damaging Bill to be passed. The Lords exist to amend legislation, and they have experts who can see the important nuances of the laws and suggest ways to improve bills. The 30% of votes that Labour lost means amendments to make the bill in question better. The 15% figure now means that the government is imposing its view and forcing its peers to vote en bloc. This is political and reduces the effectiveness of the chamber and allows bad bills to be passed.
The Bill sailed through the Commons Committee stage precisely because the Lib Dem members voted en bloc with the Tories. Not one single Labour amendment was passed by the Commons Committee. In fact not one single non-Government amendment was passed, because the Tory whips threatened Tory and Lib Dem MPs telling them that the only amendments that would be allowed to pass the Commons Committee would be those proposed by the government. This is the behaviour of a authoritarian government that believes that it is always right (a very frightening concept). We are finding the same behaviour in the Lords Committee.
If the Tories had not been handed a Coalition, and were now ruling by supply and confidence, the Lib Dem peers would be free to make amendments and make this bill better. Even if the Tories had scraped through the 2010 with a narrow majority, the Lib Dem peers would more often than not be changing this bill. Now they are sitting on their hands. It is very clear: Coalition is bad, and allows bad laws to pass.
Tuesday 8 November 2011
Choice
I attended a patient forum meeting last night at my local hospital. During his talk the Medical Director told us a joke that he said was prevalent in the NHS of the 80s:
Well, I guess the humour is all in the delivery. The point was to illustrate the "Soviet-style" of public services in the 80s: we were just too amenable to waiting long times.
Things have changed now, of course. The NHS constitution says that we have to be treated within 18 weeks and as David Cameron has found, there is a political cost to allowing waiting times to go up.
The 18 week RTT target was politically concocted, there is no special meaning to 4.5 months. (In Denmark, for example, the waiting time has to be less than 1 month.) Anyone who has been on a waiting list will tell you that it is not necessarily the amount of time that is the issue, it is the uncertainty of not knowing when you'll get the treatment. The uncertainty is especially acute if the patient is worried about the treatment.
Cutting waiting lists is expensive, so it is unlikely that any political party will promise to cut the (arbitrary) 18 week target. However, there is another policy that could be offered. Patients could be given one of two choices: treatment within 18 weeks, but the date is determined by the provider (the situation at the moment); or treatment on a date of the patient's choosing as long as it is outside the 18 week window (the actual limit may be different to 18 weeks). The idea would be to guarantee (as much it is possible to guarantee) that a patient will get the treatment on the day that is specified by the patient. This means that the patient will know that their cataracts will be replaced before they go on their birdwatching holiday, or their hip will be replaced before their child's wedding. There will be still work for NHS providers to so: they will have to have the capacity so that patients on the 18 week guarantee will fill the "gaps" between the patients who have booked.
So the joke would be partially true, patients may recieve treatment many months in the future, but the difference would be that they choose to have their treatment on that date. I think that this could be a popular policy at the next election.
Receptionist: We can give you a date for your hip replacement: it will be 10:30am on June 22nd, 2015
Patient: Sorry, but I cannot make that appointment. The Gas Board is coming to install my cooker at 11 on that day.
Well, I guess the humour is all in the delivery. The point was to illustrate the "Soviet-style" of public services in the 80s: we were just too amenable to waiting long times.
Things have changed now, of course. The NHS constitution says that we have to be treated within 18 weeks and as David Cameron has found, there is a political cost to allowing waiting times to go up.
The 18 week RTT target was politically concocted, there is no special meaning to 4.5 months. (In Denmark, for example, the waiting time has to be less than 1 month.) Anyone who has been on a waiting list will tell you that it is not necessarily the amount of time that is the issue, it is the uncertainty of not knowing when you'll get the treatment. The uncertainty is especially acute if the patient is worried about the treatment.
Cutting waiting lists is expensive, so it is unlikely that any political party will promise to cut the (arbitrary) 18 week target. However, there is another policy that could be offered. Patients could be given one of two choices: treatment within 18 weeks, but the date is determined by the provider (the situation at the moment); or treatment on a date of the patient's choosing as long as it is outside the 18 week window (the actual limit may be different to 18 weeks). The idea would be to guarantee (as much it is possible to guarantee) that a patient will get the treatment on the day that is specified by the patient. This means that the patient will know that their cataracts will be replaced before they go on their birdwatching holiday, or their hip will be replaced before their child's wedding. There will be still work for NHS providers to so: they will have to have the capacity so that patients on the 18 week guarantee will fill the "gaps" between the patients who have booked.
So the joke would be partially true, patients may recieve treatment many months in the future, but the difference would be that they choose to have their treatment on that date. I think that this could be a popular policy at the next election.
Thursday 3 November 2011
Dithering
During the second reading of the Health and Social Care Bill Lord Owen suggested that clause 1, the clause that determines the Secretary of State's responsibility, should be considered by a Select Committee of legal and health policy experts rather than the full Committee of the House. The Government claimed that this was an act to wreck the Bill and Lord Owen stressed that this was not the case, even offering to put a time limit on the Select Committee:
Lord Howe, the Government minister rejected this amendment:
Then yesterday the Government had a re-think. Commenting on the group of amendments to clause 1 being debated, Lord Howe said:
The result of this dithering means that there is now a real danger of delay in the passage of the Bill, something that Lord Owen had tried to avoid with his original amendment. There is also real danger that there will not be sufficient time to debate whatever amendments that are made to clause 1. If Howe had allowed the clause to be examined by a Select Committee there would have been an opportunity for a full debate.
Lord Howe has handled this very badly, but it is symptomatic of the entire Bill: extremely badly drafted and badly managed.
"My noble friend and I said we thought it was absolutely reasonable that to protect the business of the House they wanted this Bill before the new Session. We had already made it clear that this would have to be reported out from Select Committee by 19 December, and that was acceptable. The clerks tell me they have to report it out. They may say they want more time but there has to be a report. So I think we have dealt with one of the problems."This explicitly says that the Select Committee will report before the 19th of December.
Lord Howe, the Government minister rejected this amendment:
"The provisions that the noble Lord, Lord Owen, asks us to send to a special Select Committee affect the entire Bill. The twin-track approach that he advocates carries a major risk: the potential disconnect between the special Select Committee and the Committee of the whole House. The Select Committee might recommend amendments to parts of the Bill that have already been debated by the Committee of the whole House. The result could be that, notwithstanding the offer made in good faith by the noble Baroness, Lady Royall, we could see a slippage of the timetable of the Bill that would be most unwelcome."This basically says that Lord Howe rejected the idea of having a Select Committee because it may discuss amendments already discussed by the entire House (sitting as a Committee on the Bill) and this would delay the Bill further. The Government is desperate to ram the Bill through Parliament because if the Bill is not passed before April 2012 the timetable for major changes like abolishing PCTs and SHAs will have to be changed.
Then yesterday the Government had a re-think. Commenting on the group of amendments to clause 1 being debated, Lord Howe said:
"having spoken to a number of noble Lords during the past few days, including my noble and learned friend, it is my view that the best course for this Committee would be for none of the amendments in this group to be moved today, and instead for us to use the time between now and Report to reflect further on these matters in a spirit of co-operation."Now Lord Howe is saying that he does not want the full Committee of the House to discuss the clause, and instead he wants to submit an amendment during the Report stage of the Bill (in January). Later in the debate he added:
"I have said that I believe the balance of advantage for this Committee lies in our agreeing collectively not to amend the Bill at this stage and I am pleased that there seems to be consensus around that view. I believe instead that it would be profitable for me to engage with noble Lords in all parts of the House, both personally and with the help of my officials, between now and Report to try to reach consensus on these important matters."During the Second Reading Lord Howe said that the clause must be debated by the whole House Committee, rejecting the proposal to ask a Select Committee of experts; yet yesterday Lord Howe says that he wants informal talks with Lords rather than to allow debate in the full Committee.
The result of this dithering means that there is now a real danger of delay in the passage of the Bill, something that Lord Owen had tried to avoid with his original amendment. There is also real danger that there will not be sufficient time to debate whatever amendments that are made to clause 1. If Howe had allowed the clause to be examined by a Select Committee there would have been an opportunity for a full debate.
Lord Howe has handled this very badly, but it is symptomatic of the entire Bill: extremely badly drafted and badly managed.
Tuesday 1 November 2011
GP Market
There was a short piece on the Today programme yesterday (here at 52m52s, also on the BBC website here) where journalist Jane Dreaper interviewed Sir David Nicholson. There wasn't much discussed, but the following was interesting.
Sir David said that under the Health Bill data will be provided about what services your GP provides compared to other GPs in the area and nationally:
Then there is the issue of how will patients know what services could be available? Occasionally I attend diabetic support group meetings and it is clear that there are some people who have had diabetes for decades and are still treating it like they were first taught to. Their blood tests show that their control is adequate so there is no need to tell them to do things differently. If a patient is treating their diabetes like it is 1980, they will not know if their GP is not providing all the diabetic services they should. It should not be the responsibility of the patient to move to a GP with the best services, it should be the responsibility of all GP practices to provide all the necessary services.
The final issue with Sir David's comment is that it appears to ignore the structures that he is putting in place. Every GP has to be part of a Clinical Commissioning Group (CCG). The Health Bill says that CCGs have the responsibility to ensure that healthcare services are provided for the patients in the area that the CCG covers. This is important: it is a responsibility of the CCG that the GP practices in the group provide the services that are required for their patients. So if a GP does not provide a service that will be as much the responsibility of the CCG as the GP. To get the service the patient needs, s/he will have to move to a GP practice in another CCG that supports the service. There are some large CCGs (for example the Manchester CCG has 107 GP practices, Liverpool has 91, County Durham has 88) so moving to another GP in another CCG will mean having to change to a GP in another city. That is simply not possible for most patients and certainly not possible for patients with long term conditions who need a continuity of care.
Sir David was suggesting a market of GP, but he has structured the NHS so that this is not possible.
Sir David said that under the Health Bill data will be provided about what services your GP provides compared to other GPs in the area and nationally:
"this is a powerful mechanism for patients to make choices about which GP they use - if you have a long term condition you might want to think in the future about different GPs and whether they are providing a full range of services"There are a couple of issues that Sir David is ignoring here. First - it should not be necessary to say this, but clearly Sir David seems to have forgotten - a long term condition (LTC) is 24x7 and it is usually for life. A patient will die with the LTC and most likely will die of the LTC. This makes continuity of care vitally important. The best control of their condition comes when patients with LTCs have a good and continuing relationship with their care team. The idea that patients can simply "shop around" for services means that such relationships will be difficult to form and maintain and this threatens continuity of care. Jonathon Tomlinson has written extensively about the relationship between GPs and their patients and Sir David could do no better than to read his latest blog.
Then there is the issue of how will patients know what services could be available? Occasionally I attend diabetic support group meetings and it is clear that there are some people who have had diabetes for decades and are still treating it like they were first taught to. Their blood tests show that their control is adequate so there is no need to tell them to do things differently. If a patient is treating their diabetes like it is 1980, they will not know if their GP is not providing all the diabetic services they should. It should not be the responsibility of the patient to move to a GP with the best services, it should be the responsibility of all GP practices to provide all the necessary services.
The final issue with Sir David's comment is that it appears to ignore the structures that he is putting in place. Every GP has to be part of a Clinical Commissioning Group (CCG). The Health Bill says that CCGs have the responsibility to ensure that healthcare services are provided for the patients in the area that the CCG covers. This is important: it is a responsibility of the CCG that the GP practices in the group provide the services that are required for their patients. So if a GP does not provide a service that will be as much the responsibility of the CCG as the GP. To get the service the patient needs, s/he will have to move to a GP practice in another CCG that supports the service. There are some large CCGs (for example the Manchester CCG has 107 GP practices, Liverpool has 91, County Durham has 88) so moving to another GP in another CCG will mean having to change to a GP in another city. That is simply not possible for most patients and certainly not possible for patients with long term conditions who need a continuity of care.
Sir David was suggesting a market of GP, but he has structured the NHS so that this is not possible.
Sunday 30 October 2011
NHS Expenditure
The government keeps telling us that they will deliver real terms increases in the NHS budget, but the evidence proves otherwise. Today The Independent says that
Further, the House of Commons Library Standard Note SN/SG/724 (updated September 2011) says that Net NHS Expenditure in 2009-10 (in 2010-11 prices) was £103.2bn and in 2010-11 the expenditure was £102.0bn a real terms decrease of -1.1%.
The House of Commons library standard mote gives tables of NHS funding from when the service was created. Table 2 gives the expenditure on the NHS in England in 2010/11 prices (ie real terms) from 1974/75 to 2014/15. The last five years are the planned expenditure by the current government.The following graph shows the data plotted.

I have published a graph like this before, this new one is updated to show the new figures in the standard note (effectively, the dip seen for 2010-11). I have fitted three lines to this data, one for the Thatcher/Major years, one for Blair/Brown and the final one for the Cameron era. It is very clear that the current government is squeezing the NHS.
In the following graph I have plotted the data from 2006 with the Blair/Brown trend line plotted in blue and the Thatcher/Major trend in red. Clearly Cameron's funding is less than if the Blair/Brown spending had continued at the same rate, but what is striking is how Cameron's spending compares with Thatcher/Major. If the NHS were funded by Conservatives from the 80s we would have real terms increases of about £1bn every year, instead there is flat funding.

"NHS total expenditure [fell] from £102.8bn in 2009-10 to £102.0bn in 2010-11 (in 2010-11 prices, rounded to nearest £0.1bn) – a real terms fall of 0.7 per cent."
Further, the House of Commons Library Standard Note SN/SG/724 (updated September 2011) says that Net NHS Expenditure in 2009-10 (in 2010-11 prices) was £103.2bn and in 2010-11 the expenditure was £102.0bn a real terms decrease of -1.1%.
The House of Commons library standard mote gives tables of NHS funding from when the service was created. Table 2 gives the expenditure on the NHS in England in 2010/11 prices (ie real terms) from 1974/75 to 2014/15. The last five years are the planned expenditure by the current government.The following graph shows the data plotted.
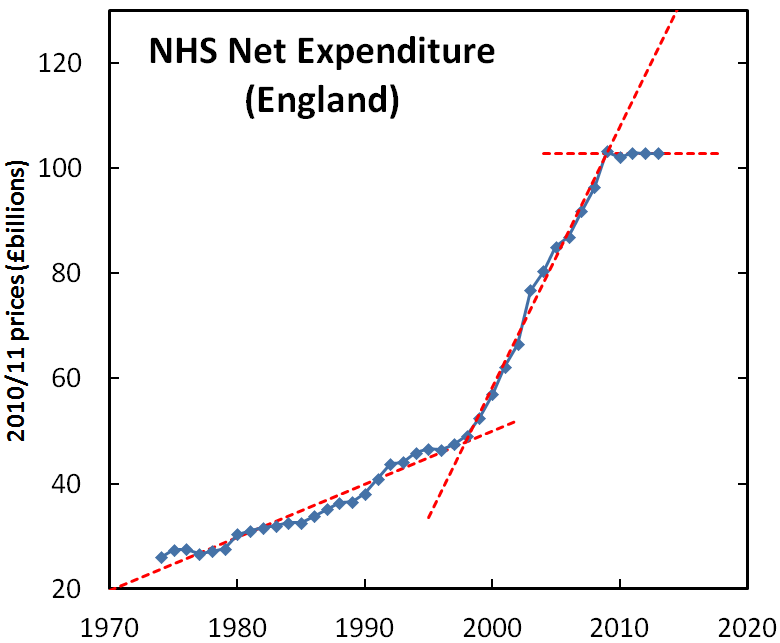
I have published a graph like this before, this new one is updated to show the new figures in the standard note (effectively, the dip seen for 2010-11). I have fitted three lines to this data, one for the Thatcher/Major years, one for Blair/Brown and the final one for the Cameron era. It is very clear that the current government is squeezing the NHS.
In the following graph I have plotted the data from 2006 with the Blair/Brown trend line plotted in blue and the Thatcher/Major trend in red. Clearly Cameron's funding is less than if the Blair/Brown spending had continued at the same rate, but what is striking is how Cameron's spending compares with Thatcher/Major. If the NHS were funded by Conservatives from the 80s we would have real terms increases of about £1bn every year, instead there is flat funding.

Saturday 29 October 2011
CCG Size: designed to fail
I have taken the data from the Department of Health for the current Clinical Commissioning Groups. The relevant figures are:
CCGs
Number of CCGs: 266
Mean population per CCG: 198,973
Median population per CCG: 167,210
PCTs
Number of PCTs: 152
Mean population per PCT: 340,900
Median population per PCT: 282,200
I have plotted out the numbers of PCTs and CCGs in various population bands:

The PCTs are in dark blue and the CCGs are in light blue. It is immediately obvious that the centre of gravity of the graph of the CCGs is much lower than for PCTs: the clinical commissioning groups are much smaller than PCTs. More concerning is that out of 266 CCGs four fifths of them (219) have populations less than 300k. (For comparison 87, or 57% of PCTs were under 300k.) Three hundred thousand is the figure given by Civitas as the rough rule of thumb for the minimum size for a commissioning group to be financially viable:
CCGs
Number of CCGs: 266
Mean population per CCG: 198,973
Median population per CCG: 167,210
PCTs
Number of PCTs: 152
Mean population per PCT: 340,900
Median population per PCT: 282,200
I have plotted out the numbers of PCTs and CCGs in various population bands:

The PCTs are in dark blue and the CCGs are in light blue. It is immediately obvious that the centre of gravity of the graph of the CCGs is much lower than for PCTs: the clinical commissioning groups are much smaller than PCTs. More concerning is that out of 266 CCGs four fifths of them (219) have populations less than 300k. (For comparison 87, or 57% of PCTs were under 300k.) Three hundred thousand is the figure given by Civitas as the rough rule of thumb for the minimum size for a commissioning group to be financially viable:
In 10 European countries analysed, seven have seen a consolidation of commissioning organisations over the past 15 to 20 years, two have seen no change. In only one country (Spain, due to devolution) has the number of commissioning organisations increased. In all countries apart from Switzerland the average population coverage of a commissioner is above 300,000 people.With so many small CCGs is GP commissioning designed to fail?
Friday 28 October 2011
The Mackay Amendment
Paul Waugh reported a few days ago that the government would "look favourably on an amendment by Lord Mackay", so I thought that I would investigate what this amendment does. Since the Bill amends several other bills the only way to understand an amendment is to follow the amendment's instructions.
The National Health Service Act 2006 starts with a clause on the responsibilities of the Secretary of State:
The Mackay amendment changes the 2006 Act to say:
The new part is in subsection 2(s). To explain its significance let's go back to Baroness Williams' opposition to the Bill at the Lib Dem conference in September. The Baroness said that a "major health emergency in the country was an example of when the secretary of state's role was unclear". Section 2(b) and section 4 explains the intervention that the Secretary of State is able to make in an emergency.
Section 4 lists several sections from the H&SC Bill and several existing acts. Section 13Z1 (a new section added to the NHS 2006 Act by the H&SC Bill) says that the Secretary of State can intervene if he considers that the NHS Commissioning Board has failed to discharge its duties and similarly section 82 of the Health and Social Care Act 2008 says that the Secretary of State can intervene if the Care Quality Commission fails to discharge its functions.
Section 253 of the 2006 Act says that the Secretary of State can intervene in a service in an emergency, but crucially Foundation Trusts are excluded. Section 67, 242, 266 and 285 of the Health and Social Care Bill already say that the SoS can intervene if one of these bodies (Monitor, NICE, the Health and Social Care Information Centre) fails, or if these bodies fail to co-operate with each other.
Section 4 of the Mackay amendment says nothing new, it merely lists existing sections in the new Bill or sections in existing acts when the Secretary of State can intervene. I cannot see that we gain anything by having the Mackay amendment, so I fail to understand why Lib Dem would consider this as a solution.
The National Health Service Act 2006 starts with a clause on the responsibilities of the Secretary of State:
1 Secretary of State's duty to promote health service
(1) The Secretary of State must continue the promotion in England of a comprehensive health service designed to secure improvement—The current version of the Health and Social Care Bill will change this clause to:
(a) in the physical and mental health of the people of England, and
(b) in the prevention, diagnosis and treatment of illness.
(2) The Secretary of State must for that purpose provide or secure the provision of services in accordance with this Act.
(3) The services so provided must be free of charge except in so far as the making and recovery of charges is expressly provided for by or under any enactment, whenever passed.
1 Secretary of State’s duty to promote comprehensive health service
(1) The Secretary of State must continue the promotion in England of a comprehensive health service designed to secure improvement—Note that subsection of the 2006 Act says "must for that purpose provide or secure the provision of services" and this is amended to "must exercise the functions conferred by this Act so as to secure that services are provided". The contentious point is the removal of the requirement to provide, the implication is that the Secretary of State will no longer provide health services.
(a) in the physical and mental health of the people of England, and
(b) in the prevention, diagnosis and treatment of illness.
(2) For that purpose, the Secretary of State must exercise the functions conferred by this Act so as to secure that services are provided in accordance with this Act.
(3) The services provided as part of the health service in England must be free of charge except in so far as the making and recovery of charges is expressly provided for by or under any enactment, whenever passed.
The Mackay amendment changes the 2006 Act to say:
1 Secretary of State's duty to promote health service
(1) The Secretary of State must continue the promotion in England of a comprehensive health service designed to secure improvement—The changes are subsection 2 and 4. This splits the responsibility into two. The first part says that Lansley has the ultimate responsibility for the provision of health services. This clashes with clause 4 which says that the Secretary of State must promote autonomy of the health service. I suspect that clause 2(a) will not be accepted because to do so would require that the autonomy clause is removed, and this is known to be one of Lansley's red lines.
(a) in the physical and mental health of the people of England, and
(b) in the prevention, diagnosis and treatment of illness.
2) For that purpose, the Secretary of State—(3) The services so provided must be free of charge except in so far as the making and recovery of charges is expressly provided for by or under any enactment, whenever passed.
(a) retains ultimate responsibility to parliament for the provision of the health service in England, and
(b) must exercise the intervention and other functions of the Secretary of State in relation to that health service so as to secure that services are provided in accordance with this Act.
(4) For the purposes of this section, the intervention functions of the Secretary of State in relation to the health service in England are the functions of the Secretary of State under—
(a) section 13Z1 (failure by the Board to discharge any of its functions),
(b) section 253 (emergency powers),
(c) section 82 of the Health and Social Care Act 2008 (failure by Care Quality Commission to discharge functions),
(d) section 67 of the Health and Social Care Act 2011 (Monitor: failure to perform functions),
(e) section 242 of that Act (failure by NICE to discharge any of its functions),
(f) section 266 of that Act (failure by the Information Centre to discharge any of its functions), and
(g) section 285 of that Act (breaches of duties to co-operate).
The new part is in subsection 2(s). To explain its significance let's go back to Baroness Williams' opposition to the Bill at the Lib Dem conference in September. The Baroness said that a "major health emergency in the country was an example of when the secretary of state's role was unclear". Section 2(b) and section 4 explains the intervention that the Secretary of State is able to make in an emergency.
Section 4 lists several sections from the H&SC Bill and several existing acts. Section 13Z1 (a new section added to the NHS 2006 Act by the H&SC Bill) says that the Secretary of State can intervene if he considers that the NHS Commissioning Board has failed to discharge its duties and similarly section 82 of the Health and Social Care Act 2008 says that the Secretary of State can intervene if the Care Quality Commission fails to discharge its functions.
Section 253 of the 2006 Act says that the Secretary of State can intervene in a service in an emergency, but crucially Foundation Trusts are excluded. Section 67, 242, 266 and 285 of the Health and Social Care Bill already say that the SoS can intervene if one of these bodies (Monitor, NICE, the Health and Social Care Information Centre) fails, or if these bodies fail to co-operate with each other.
Section 4 of the Mackay amendment says nothing new, it merely lists existing sections in the new Bill or sections in existing acts when the Secretary of State can intervene. I cannot see that we gain anything by having the Mackay amendment, so I fail to understand why Lib Dem would consider this as a solution.
Wednesday 26 October 2011
Privatisation
OECD defines privatisation as:
This brings me onto the first definition that Lansley gave:
The House of Lords Select Committee on the Constitution says that the Bill will change the 2006 NHS Act to say:
Under Lansley's very restricted definition of privatisation, "having to pay for their care" such a charge for "hotel services" would be privatisation. When such charges are imposed (and they will be, somewhere in the country in the next few years) I wonder if Lansley will admit that the NHS in that area have been "privatised"?
Further, note the statement "we are not going to move to a place where there is any additional payment". This is happening now! The doctorpreneur GPs in Haxby told their patients that the NHS would no longer fund certain treatments (as CCGs will be able to do in the future) and then gave the patients a price list for having the treatment carried out privately additional payments for care. So under Lansley's definition privatisation has already happened in Haxby.
Update:
The question about privatisation (with a reference to Bill Clinton and cigars) from Dr Pete Deveson can be found here (at 9:38). Lansley responds to the question with a disdainful shake of the head.
Privatisation refers to transfer of ownership and control of government or state assets, firms and operations to private investors.At the RCGP conference this year Andrew Lansley was asked to define privatisation. He gave two definitions. After being challenged by Dr Clare Geralda Lansley gave the follwoing (his second definition):
Privatisation is the transfer of public service responsibilities into the private sector - we are not transferring responsibility for the NHS into the private sector.This is not the OECD definition, who say that it is the transfer of the ownership of assets as well as the control of those assets. Lansley talks about the responsibility for the NHS which is a much wider issue. The government/NHS Commissioning Board can still be responsible for the NHS even if all the assets are owned by the private sector, because in Lansley's mind the NHS is the source of the money to pay for treatment: the taxpayer.
This brings me onto the first definition that Lansley gave:
As far as the public are concerned, privatisation would mean - if you would ask them - having to pay for their care instead of receiving that care provided by the NHS free-at-the-point-of-use based on their need. We are not going to move to a place where there is any additional payment.Again, this is very different to the OECD definition, which says nothing about how services are funded.
The House of Lords Select Committee on the Constitution says that the Bill will change the 2006 NHS Act to say:
(1) A clinical commissioning group [CCG] must arrange for the provision of the following to such extent as it considers necessary to meet the reasonable requirements of the persons for whom it has responsibility—Currently the Secretary of State determines what services will be funded by the NHS, Lansley does not want this responsibility and so it will be local Clinical Commissioning Groups who will decide. The CCGs will decide based on the amount of funding they have - if they do not have enough money they may have to prioritise urgent care and may decide that services that are less "medical" should be paid for by the patient. For example hospital "hotel services". A CCG could argue that if you were not in hospital you would be paying for food and accommodation, they could argue that "hotel services" are not a medical need and so you should have to pay for them when you are admitted to hospital. This argument has been made for many years, but it is usually opposed by arguing that without the "hotel services" the patient cannot get the treatment.
(a) hospital accommodation,
(b) other accommodation for the purpose of any service provided under this Act,
(c) medical, dental, ophthalmic, nursing and ambulance services,
etc
Under Lansley's very restricted definition of privatisation, "having to pay for their care" such a charge for "hotel services" would be privatisation. When such charges are imposed (and they will be, somewhere in the country in the next few years) I wonder if Lansley will admit that the NHS in that area have been "privatised"?
Further, note the statement "we are not going to move to a place where there is any additional payment". This is happening now! The doctorpreneur GPs in Haxby told their patients that the NHS would no longer fund certain treatments (as CCGs will be able to do in the future) and then gave the patients a price list for having the treatment carried out privately additional payments for care. So under Lansley's definition privatisation has already happened in Haxby.
Update:
The question about privatisation (with a reference to Bill Clinton and cigars) from Dr Pete Deveson can be found here (at 9:38). Lansley responds to the question with a disdainful shake of the head.
Monday 24 October 2011
Personal Budgets
Ideologically I am against personal healthcare budgets. Years ago when I first explained to an American colleague why the NHS was so special I told him: "because whatever condition I have the NHS will give me treatment according to clinical need". Personal budgets go against that principle because it gives a hard cash settlement that specifies how much your condition is allowed to cost. I know that there will be assurances from the government and from Prospect-buying Blairites that no one with a personal budget will be denied care if their budget runs out, but we all know that the whole point of budgets is to give an upper limit beyond which you are not supposed to go: a financial constraint, not a clinical one. We also have to question why, at a time of austerity when the NHS has to save money, the government are forging ahead with a policy that will be more costly to administer and which (if we accept their reassurances) potentially cost more than now? The reason, as we all know, is that personal budgets allows the government to put a limit on what the NHS will pay a limit that the government can lower. This is the first step towards co-pay and top-ups. One third of patients who use the NHS have long term conditions and they use two thirds of the NHS budget; it is statistics like this get management consultants thinking, and their "solution" is personal budgets.
However, Lansley has now promised me a personal budget. I have a stable, but long term condition which means that I am exactly the target for a personal budget. At the Conservative party conference this year Lansley said that personal budgets would start in 2014. The Department of Health spin machine reports:
Since I will have to have a personal budget soon I decided to ask my local Foundation Trust what they intend to do to tailor their services for patients with personal budgets. Their reply was "I think personal budgets will be for people needing mental health care". I pursued with my questioning, pointing out what Lansley had said at the Tory party conference. It was clear to me from their response that the Foundation Trust hadn't thought about how it would change in the face of personal budgets, so here is a suggestion.
As a diabetic, I use a range of services, from top to bottom: eye checks to monitor my retinopathy; blood pressure checks (and medication); blood sugar tests (both finger prick glucose testing and HbA1c long term tests); kidney function tests (dipstick urine tests) and checks on my feet to monitor any nerve damage in the extremities. These are services I use at the moment. In the future there will be services treating heart disease and sexual dysfunction.
When I get a personal budget my GP (or a.n.other, it is not clear yet who will adjudicate) will collate the list of conditions I have and the list of preventative treatment and monitoring I need, and using the national tariff he will present me with a figure (in real cash or some made up currency) what my condition will cost every year. I will then be expected to go on a shopping trip with this budget. It is not yet clear whether I will hand my NHS Personal Budget "credit card" to each provider when I use their services, or whether I will "commission" the services off them and hence give an intention of developing a more long term relationship.
Some of the services are naturally primary care services: checks on blood pressure, kidney function and on my feet can clearly be done by a diabetic nurse or a healthcare assistant. Some services could be either in primary care or in hospital, for example monitoring of retinopathy. (Currently I am offered this service by my optician, GP and the local hospital; I choose the latter because I have had haemorrhages and a lot of laser treatment and I would prefer the monitoring to be done by a consultant.) Other services (like laser treatment for retinopathy) will be only provided by a hospital, but there is always the choice of several hospitals.
I do not look forward to the prospect of deciding who does what. This is where the FT can help. The FT could provide a care package. That is, they could put together a collection of services for people with personal budgets which would be a mixture of primary care, hospital care, and community services. These packages should have some flexibility in them (for example, I would prefer to have blood taken at my GP - because it does not involve a bus journey and the hospital does - but I would prefer the diabetologist at the hospital to interpret the results). The idea is to put together a list of services that most people use and provide an advocate who will facilitate the providers to work together for the patient. Such a care package could be put together by a GP, but in this example I will assume it is the FT that designs the package.
The advantage to the hospital is clear, they would be able to make patients aware of their services, and at the very least get some income from the administration fee for helping patients to choose. For the patient there will be an advocate who will help them choose, and will also be there throughout the year to give advice if the patient has a problem with the providers. (For example, if I am told to have my eyes monitored every 6 months and it is now 8 months since my last appointment, the advocate will chase up the appointment for me. If the advocate works for the hospital and the eye monitoring is carried out by the hospital it is more likely that the appointment issue will be resolved.) The advantage for primary care is that they will be able to provide some of the services and with closer working with the local hospital they will; provide such services cheaper.
A care package will be much better for the patient not least because the patient will not have the effort of choosing the services themselves. And the closer working between the providers that a care package will offer will help forge the mythical "integration" that the NHS is seeking.
However, Lansley has now promised me a personal budget. I have a stable, but long term condition which means that I am exactly the target for a personal budget. At the Conservative party conference this year Lansley said that personal budgets would start in 2014. The Department of Health spin machine reports:
"People receiving continuing healthcare support from the NHS will have the right to ask for a personal health budget, by April 2014 Health Secretary Andrew Lansley announced today. ... The announcement follows the independent NHS Future Forum report which recommended action to promote personal budgets and implement them within five years to give patients access to tailored services."So the personal budget programme will start with people who need continuing care (mostly elderly people) from 2014 and then before 2016 everyone with a long term condition (that includes me) will have one. (I do not think "have the right to ask for" means that you can choose not to have a personal budget because running two systems side-by-side will be too expensive and it is clear which one the government prefers patients to use.)
Since I will have to have a personal budget soon I decided to ask my local Foundation Trust what they intend to do to tailor their services for patients with personal budgets. Their reply was "I think personal budgets will be for people needing mental health care". I pursued with my questioning, pointing out what Lansley had said at the Tory party conference. It was clear to me from their response that the Foundation Trust hadn't thought about how it would change in the face of personal budgets, so here is a suggestion.
As a diabetic, I use a range of services, from top to bottom: eye checks to monitor my retinopathy; blood pressure checks (and medication); blood sugar tests (both finger prick glucose testing and HbA1c long term tests); kidney function tests (dipstick urine tests) and checks on my feet to monitor any nerve damage in the extremities. These are services I use at the moment. In the future there will be services treating heart disease and sexual dysfunction.
When I get a personal budget my GP (or a.n.other, it is not clear yet who will adjudicate) will collate the list of conditions I have and the list of preventative treatment and monitoring I need, and using the national tariff he will present me with a figure (in real cash or some made up currency) what my condition will cost every year. I will then be expected to go on a shopping trip with this budget. It is not yet clear whether I will hand my NHS Personal Budget "credit card" to each provider when I use their services, or whether I will "commission" the services off them and hence give an intention of developing a more long term relationship.
Some of the services are naturally primary care services: checks on blood pressure, kidney function and on my feet can clearly be done by a diabetic nurse or a healthcare assistant. Some services could be either in primary care or in hospital, for example monitoring of retinopathy. (Currently I am offered this service by my optician, GP and the local hospital; I choose the latter because I have had haemorrhages and a lot of laser treatment and I would prefer the monitoring to be done by a consultant.) Other services (like laser treatment for retinopathy) will be only provided by a hospital, but there is always the choice of several hospitals.
I do not look forward to the prospect of deciding who does what. This is where the FT can help. The FT could provide a care package. That is, they could put together a collection of services for people with personal budgets which would be a mixture of primary care, hospital care, and community services. These packages should have some flexibility in them (for example, I would prefer to have blood taken at my GP - because it does not involve a bus journey and the hospital does - but I would prefer the diabetologist at the hospital to interpret the results). The idea is to put together a list of services that most people use and provide an advocate who will facilitate the providers to work together for the patient. Such a care package could be put together by a GP, but in this example I will assume it is the FT that designs the package.
The advantage to the hospital is clear, they would be able to make patients aware of their services, and at the very least get some income from the administration fee for helping patients to choose. For the patient there will be an advocate who will help them choose, and will also be there throughout the year to give advice if the patient has a problem with the providers. (For example, if I am told to have my eyes monitored every 6 months and it is now 8 months since my last appointment, the advocate will chase up the appointment for me. If the advocate works for the hospital and the eye monitoring is carried out by the hospital it is more likely that the appointment issue will be resolved.) The advantage for primary care is that they will be able to provide some of the services and with closer working with the local hospital they will; provide such services cheaper.
A care package will be much better for the patient not least because the patient will not have the effort of choosing the services themselves. And the closer working between the providers that a care package will offer will help forge the mythical "integration" that the NHS is seeking.
Cherry picking
The Croydon List is study performed by the London Health Observatory and the Croydon PCT in 200x to determine how much can be saved by not performing cosmetic and ineffectual procedures.
The Croydon List also includes those procedures that have a clinical benefit but are performed when there is a "close benefit/risk balance in mild cases", or to put it in ordinary English, the patient is not yet blind enough, or in enough pain, to benefit from the operation. Let me give you some procedures that are in the ten most common procedures on the Croydon List:
You can see from this that according to the Croydon List varicose veins operations are considered low clinical value (money can be saved by not doing up to 80% of those that are done now) and that savings can be made on the others by not performing "milder" cases.
The reason whey I mention this is because HealthInvestor (a magazine for private sector healthcare) reports a paper in BMJ that says that "patients undergoing surgery in independent sector treatment centres (ISTCs) have slightly better outcomes than patients treated by NHS centres" and HealthInvestor gives the conclusion that these results "lessen concerns that ISTCs are 'cherry picking'".
However, this is exactly what the ISTCs have done because "The study reviewed the outcomes of patients undergoing hip or knee replacement, inguinal hernia repair and treatment for varicose veins across 25 ISTCs and 72 NHS providers in England". That is, they are procedures that the Croydon List says are either of little clinical use, or where cases can be considered not to be severe enough to be treated. If they are on the Croydon List it does show that ISTCs have cherry-picked the easier procedures to perform.
The Croydon List also includes those procedures that have a clinical benefit but are performed when there is a "close benefit/risk balance in mild cases", or to put it in ordinary English, the patient is not yet blind enough, or in enough pain, to benefit from the operation. Let me give you some procedures that are in the ten most common procedures on the Croydon List:
| Procedure | Min Reduction | Max Reduction |
| Inguinal hernia | 25% | 50% |
| Hip | 15% | 30% |
| Knees | 15% | 30% |
| Varicose veins | 20% | 80% |
You can see from this that according to the Croydon List varicose veins operations are considered low clinical value (money can be saved by not doing up to 80% of those that are done now) and that savings can be made on the others by not performing "milder" cases.
The reason whey I mention this is because HealthInvestor (a magazine for private sector healthcare) reports a paper in BMJ that says that "patients undergoing surgery in independent sector treatment centres (ISTCs) have slightly better outcomes than patients treated by NHS centres" and HealthInvestor gives the conclusion that these results "lessen concerns that ISTCs are 'cherry picking'".
However, this is exactly what the ISTCs have done because "The study reviewed the outcomes of patients undergoing hip or knee replacement, inguinal hernia repair and treatment for varicose veins across 25 ISTCs and 72 NHS providers in England". That is, they are procedures that the Croydon List says are either of little clinical use, or where cases can be considered not to be severe enough to be treated. If they are on the Croydon List it does show that ISTCs have cherry-picked the easier procedures to perform.
Yet Another Lansley U-turn?
I thought it was a mistake for John Healey to be so effusive about Lansley in his speech to the Kings Fund earlier this year. In that speach Healey said
One example of this is GP practice boundaries. Consistently, over the last year, Lansley has defended his plan to give patients choice over GPs. A year ago, this choice could be any GP anywhere in England, which lead to some commentators speculating that GPs who looked favourably on complimentary treatments would get patients from all over the country. Lansley had deliberately avoided mandating that GP Consortia should cover practices from a geographical area so it could have been possible for a consortia to cover GP practices from all over the country. The Future Forum recognised that this was nonsense and reluctantly Lansley changed this policy to say that Clinical Commissioning Groups must cover a geographical area and preferably those practices within a local authority boundaries.
The issue of practice boundary (rather than commissioning group boundaries) has raged on for a year now. Fairly early on it became clear that abolishing GP boundaries would have a knock-on effect on the planned 111 urgent service. The problem is that if a patient needs a home visit from their GP this would be completely impractical if the patient is not local to the GP. So the 111 urgent service had to changed to cover patients in a geographical area effectively replicating the GP home visiting service provided by GPs. Lansley's intransigence on GP boundaries was adding expense to the new 111 service.
GP boundaries have an effect on commissioning. If a GP practice can have patients from any area this means that the Clinical Commissioning Group that contains the GP practice will not cover a population in a defined area. Local services commissioned by the CCG will by necessity cover a geographical area, but with a disparate patient list these would be difficult to commission. GP boundaries also have a significant effect on funding. If patients have a choice of GPs they may "shop around" for the GPs with the higher budgets. If a practice has a patient with an expensive long term condition this will mean less money for other patients, this may mean that other patients will move away to practices without expensive patients. If patients move from a practice this will compound the problem because as a practice patient list shrinks the expensive patients will take up progressively more of the shrinking budget. Abolishing practice boundaries will make it more likely that GP practices will go bankrupt.
A lot of GPs have been worried about the practice boundary issue because it is the essence of risk pooling: the money not spent on health patients can be spent on patients with health problems. At the RCGP Annual Conference last week Lansley was challenged on GP boundaries and issued what is clearly a u-turn (Pulse):
This is clearly a case of incompetence, abolishing practice boundaries was never a policy that could work while GP practices are paid through a capitation (a fixed fee per registered patient). Abolishing practice boundaries may work if patients with expensive conditions are given personal healthcare budgets, but at the moment no one knows how, or whether, personal budgets will work, and currently they are unpopular with patients as a way to fund healthcare.
It really is time that Labour stopped praising Lansley for his "knowledge" of the NHS and start criticising him for forcing on us an incompetent policy. As one comment on the Pulse article says:
"No-one in the House of Commons knows more about the NHS than Andrew Lansley – except perhaps Stephen Dorrell. But Andrew Lansley spent six years in Opposition as shadow health secretary. No-one has visited more of the NHS. No-one has talked to more people who work in the NHS than Andrew Lansley."Healey went on to say that "these are the wrong reforms at the wrong time", but the damage had been done, from this point onwards the Prime Minister would quote the first part "no-one knows more about the NHS than Lansley" and not the latter part "these are the wrong reforms at the wrong time". It was incompetent speech writing to compliment Lansley in any way at all, for he is wreaking irreparable damage to the NHS. And what's more, Lansley is extremely incompetent having entered the Department of Health with a totally unworkable policy that has had to be mutilated to make it work, replacing the existing workable policies with policies that barely work.
One example of this is GP practice boundaries. Consistently, over the last year, Lansley has defended his plan to give patients choice over GPs. A year ago, this choice could be any GP anywhere in England, which lead to some commentators speculating that GPs who looked favourably on complimentary treatments would get patients from all over the country. Lansley had deliberately avoided mandating that GP Consortia should cover practices from a geographical area so it could have been possible for a consortia to cover GP practices from all over the country. The Future Forum recognised that this was nonsense and reluctantly Lansley changed this policy to say that Clinical Commissioning Groups must cover a geographical area and preferably those practices within a local authority boundaries.
The issue of practice boundary (rather than commissioning group boundaries) has raged on for a year now. Fairly early on it became clear that abolishing GP boundaries would have a knock-on effect on the planned 111 urgent service. The problem is that if a patient needs a home visit from their GP this would be completely impractical if the patient is not local to the GP. So the 111 urgent service had to changed to cover patients in a geographical area effectively replicating the GP home visiting service provided by GPs. Lansley's intransigence on GP boundaries was adding expense to the new 111 service.
GP boundaries have an effect on commissioning. If a GP practice can have patients from any area this means that the Clinical Commissioning Group that contains the GP practice will not cover a population in a defined area. Local services commissioned by the CCG will by necessity cover a geographical area, but with a disparate patient list these would be difficult to commission. GP boundaries also have a significant effect on funding. If patients have a choice of GPs they may "shop around" for the GPs with the higher budgets. If a practice has a patient with an expensive long term condition this will mean less money for other patients, this may mean that other patients will move away to practices without expensive patients. If patients move from a practice this will compound the problem because as a practice patient list shrinks the expensive patients will take up progressively more of the shrinking budget. Abolishing practice boundaries will make it more likely that GP practices will go bankrupt.
A lot of GPs have been worried about the practice boundary issue because it is the essence of risk pooling: the money not spent on health patients can be spent on patients with health problems. At the RCGP Annual Conference last week Lansley was challenged on GP boundaries and issued what is clearly a u-turn (Pulse):
He said: 'I'm clear that whatever we do, general practice must always remain rooted in local communities. We need to think carefully about how to manage home visiting, about how patients who don't live locally to their practice can receive urgent care, and about how information is shared. We will make sure it is done in a way that will preserve the responsibility for CCGs for the health of their local population.' When pushed to clarify his position, Mr Lansley said: 'I am not abolishing, or about abolishing, practice boundaries. I am intending to extend patient choice.'Clearly his position has changed. For a year now he has insisted that practice boundaries were 'a solid wall of defence' against patient choice and therefore he had to remove them. Now Lansley is admitting that boundaries must be retained but now he needs to 'think carefully' on how to extend patient choice of GPs.
This is clearly a case of incompetence, abolishing practice boundaries was never a policy that could work while GP practices are paid through a capitation (a fixed fee per registered patient). Abolishing practice boundaries may work if patients with expensive conditions are given personal healthcare budgets, but at the moment no one knows how, or whether, personal budgets will work, and currently they are unpopular with patients as a way to fund healthcare.
It really is time that Labour stopped praising Lansley for his "knowledge" of the NHS and start criticising him for forcing on us an incompetent policy. As one comment on the Pulse article says:
"This is another example of how Lansley has no idea how the system works at a grassroots level. Words alone fail me when trying to express how fundamentally flawed Mr Lansley and his health bill are, and just how deluded and misguided he is! He simply does not have the knowledge, competance or experience to usher in this "top down" reorganisation of the NHS - something which his party's manifesto pledged it would not undertake."This says it all, Labour needs to echo these sentiments: Lansley is incompetent.
Subscribe to:
Posts (Atom)





